

Predictors of treatment attendance in cognitive and dynamic therapies for major depressive disorder delivered in a community mental health setting
- PMID: 31204838
- PMCID: PMC6768545
- DOI: 10.1037/ccp0000414
Predictors of treatment attendance in cognitive and dynamic therapies for major depressive disorder delivered in a community mental health setting
Abstract
Objective: Our goal was to evaluate treatment attendance patterns, including both treatment completion and premature termination from treatment, for 2 evidence-based psychotherapies for major depressive disorder (MDD) delivered in a community mental health setting. We explored rates of premature termination across the course of treatment as well as the factors that predicted and moderated premature termination and treatment completion.
Method: This investigation included 237 patients with MDD who participated in a noninferiority trial comparing short-term dynamic psychotherapy (DT) to cognitive therapy (CT). Patients in both conditions were offered 16 sessions of treatment and had up to 5 months to complete treatment. All patients completed an extensive self-report battery at treatment baseline as well as measures of the therapeutic alliance and opinions about treatment following Session 2.
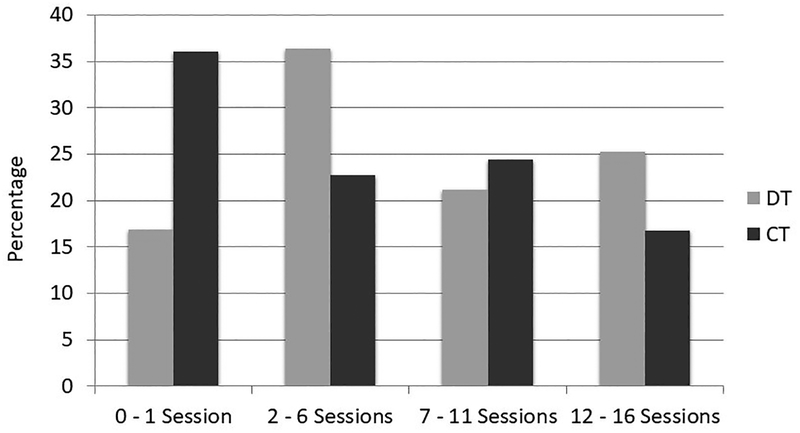
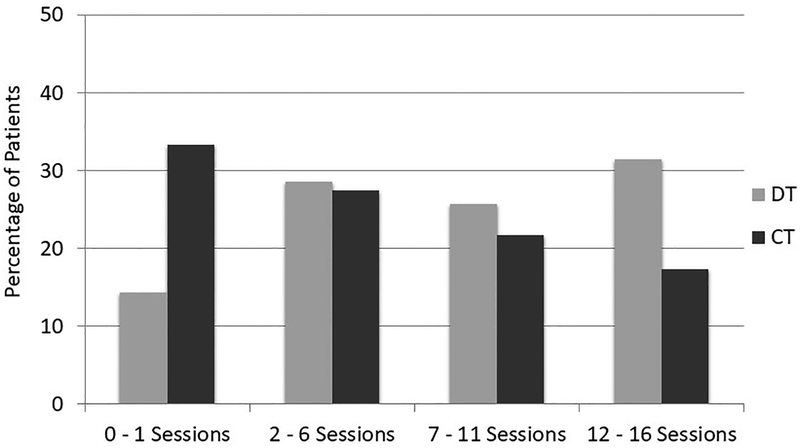
Results: Premature termination from both treatments was high with 27% of patients discontinuing treatment very early after only an intake session or a single treatment session. Patients in CT were significantly more likely to terminate treatment prematurely, χ²(3) = 14.35, p = .002. Baseline physical health functioning, subthreshold psychotic symptoms, Session 2 ratings of agreement on tasks, and Session 2 ratings of treatment sensibility all independently predicted premature termination of services. Trauma history significantly moderated very early termination of treatment, χ²(3) = 10.26, p = .017, with patients with high trauma histories more likely to complete DT but terminate prematurely from CT.
Conclusions: Very early termination from services was higher in CT compared with DT. Including techniques to improve engagement in both therapies and matching patients to treatment based on predictors/moderators may be effective ways to optimize treatment engagement. (PsycINFO Database Record (c) 2019 APA, all rights reserved).
Figures
References
-
- American Psychiatric Association. (2002). Multiaxial assessment In DSM-IV-TR: Diagnostic and Statistical Manual of Mental Disorders (4th ed., text revision). Washington, DC: American Psychiatric Association.
-
- Andersen RM (1968). Behavioral model of families’ use of health services research (Series No. 25). Chicago: Center for Health Administration Studies, University of Chicago.
-
- Andersen RM (1995). Revisiting the behavioral model and access to medical care: Does it matter? Journal of Health and Social Behavior, 36, 1–10. - PubMed
-
- Babor TF, de la Fuente JR, Saunders J, & Grant M (1989). The Alcohol Use Disorders Identification Test: Guidelines for Use in the Primary Health Care. WHO Publication No. 89.4, Geneva: World Health Organization.
-
- Babor TF, Higgins-Biddle JC, Saunders JB, Monteiro MG, & World Health Organization. Dept. of Mental Health and Substance Dependence. (2001). AUDIT: The Alcohol Use Disorders Identification Test: Guidelines for use in primary health care, 2nd ed. Geneva: World Health Organization.
