

SREAT presenting as decades of intractable seizures and isolated delusional episodes with clinical, laboratory, and EEG confirmation of treatment response
- PMID: 31205712
- PMCID: PMC6537057
- DOI: 10.1177/2050313X19850051
SREAT presenting as decades of intractable seizures and isolated delusional episodes with clinical, laboratory, and EEG confirmation of treatment response
Abstract
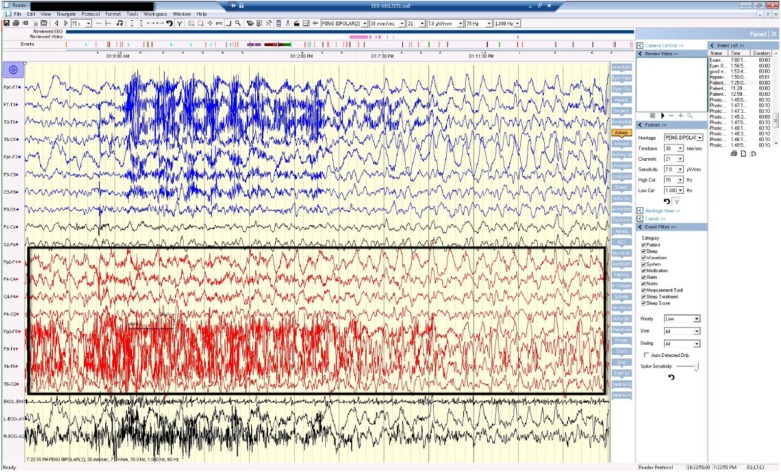
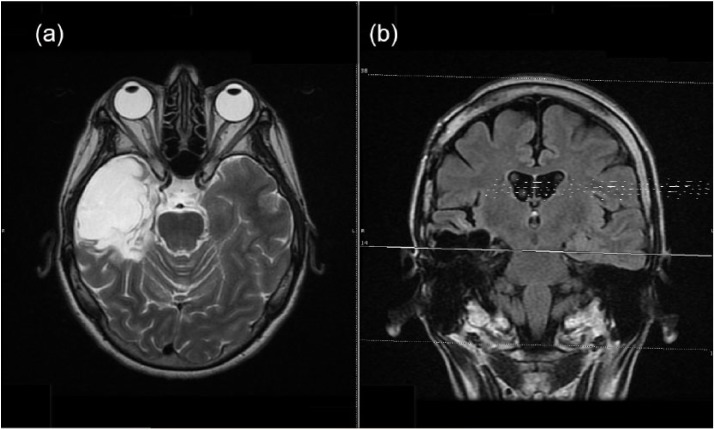
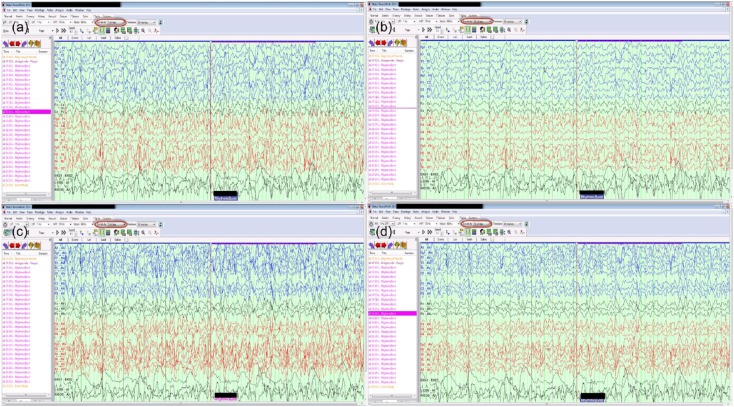
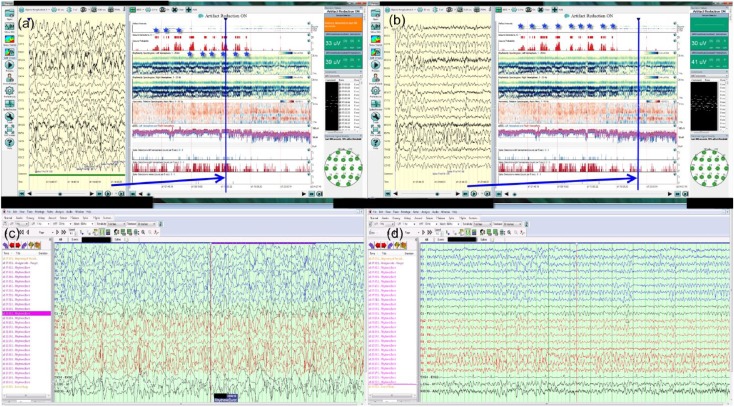
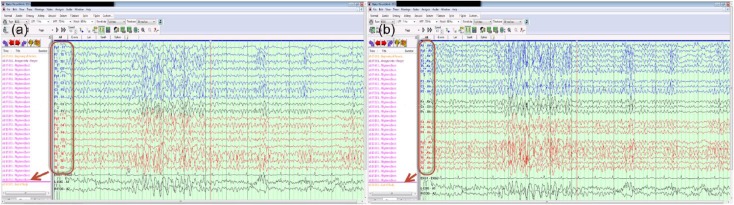
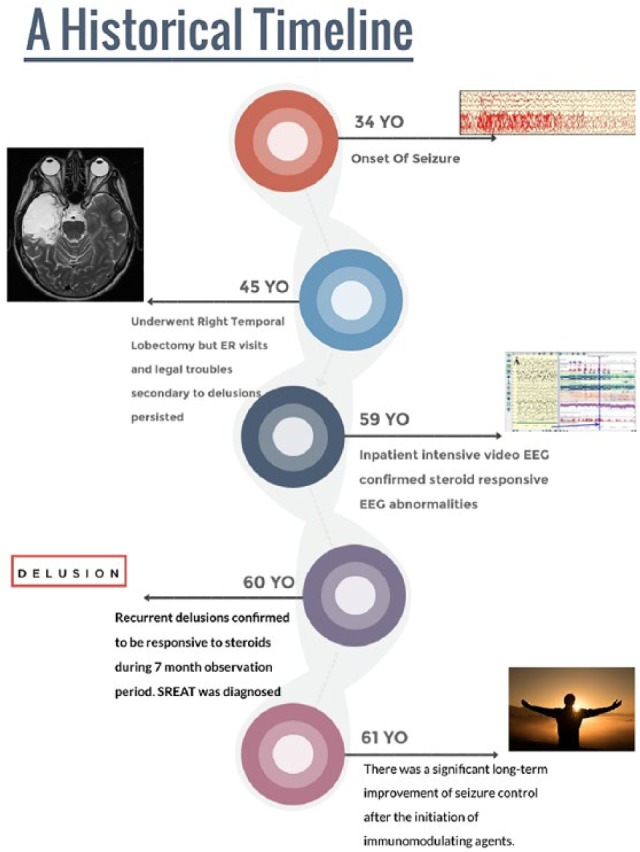
We report a case of a 60-year-old woman with a history of intractable seizures and isolated delusional psychosis who was later diagnosed with steroid-responsive encephalopathy associated with autoimmune thyroiditis. The patient underwent right temporal lobectomy (epilepsy surgery) 15 years before coming to this clinic, but continued to have focal seizures, resulting in frequent emergency room visits thereafter. After admission for intensive inpatient video electroencephalogram monitoring and subsequent 7 months of close follow-up, both the electroencephalogram abnormalities and isolated delusional psychosis were found to be responsive to immunotherapy. This suggests that her epilepsy may be autoimmune in nature. Steroid-responsive encephalopathy associated with autoimmune thyroiditis was diagnosed after 26 years since the onset of seizures. Performing invasive epilepsy surgery in patients with autoimmune epilepsy cannot reverse the inflammatory process; therefore, it is reasonable to test for autoimmune etiologies before excision surgery on patients with medically intractable epilepsy. This case demonstrates the clinical use of quantitative electroencephalogram in assisting with the diagnosis of steroid-responsive encephalopathy associated with autoimmune thyroiditis and supports that it is a spectrum disorder with protean manifestations.
Keywords: Hashimoto’s encephalopathy; Steroid-responsive encephalopathy associated with autoimmune thyroiditis; thyroglobulin antibody; thyroperoxidase antibody.
Conflict of interest statement
Declaration of conflicting interests: The author(s) declared no potential conflicts of interest concerning the research, authorship, and publication of this article.
Figures
Similar articles
-
Recurrent partial seizures with ictal yawning as atypical presentation of Hashimoto's encephalopathy (steroid-responsive encephalopathy associated with autoimmune thyroiditis).Epilepsy Behav. 2011 Dec;22(4):799-803. doi: 10.1016/j.yebeh.2011.09.023. Epub 2011 Oct 24. Epilepsy Behav. 2011. PMID: 22030535
-
Steroid-Responsive Encephalopathy Associated With Autoimmune Thyroiditis Presenting With Parkinsonism.Cureus. 2024 Mar 14;16(3):e56184. doi: 10.7759/cureus.56184. eCollection 2024 Mar. Cureus. 2024. PMID: 38618344 Free PMC article.
-
An Intriguing Case of Delirium: Recognizing Steroid-Responsive Encephalopathy Associated With Autoimmune Thyroiditis.Cureus. 2024 Sep 29;16(9):e70447. doi: 10.7759/cureus.70447. eCollection 2024 Sep. Cureus. 2024. PMID: 39473654 Free PMC article.
-
Steroid responsive encephalopathy associated with autoimmune thyroiditis (SREAT) in childhood.J Pediatr Endocrinol Metab. 2014 Jul;27(7-8):737-44. doi: 10.1515/jpem-2013-0435. J Pediatr Endocrinol Metab. 2014. PMID: 24598831 Review.
-
Thyroid gland and brain: Enigma of Hashimoto's encephalopathy.Best Pract Res Clin Endocrinol Metab. 2019 Dec;33(6):101364. doi: 10.1016/j.beem.2019.101364. Epub 2019 Nov 23. Best Pract Res Clin Endocrinol Metab. 2019. PMID: 31801687 Review.
Cited by
-
Diagnostic and Therapeutic Challenges of Steroid-Responsive Encephalopathy Associated With Thyroiditis: A Case Report.Cureus. 2024 Jul 25;16(7):e65369. doi: 10.7759/cureus.65369. eCollection 2024 Jul. Cureus. 2024. PMID: 39184674 Free PMC article.
References
-
- Laurent C, Capron J, Quillerou B, et al. Steroid-responsive encephalopathy associated with autoimmune thyroiditis (SREAT): characteristics, treatment and outcome in 251 cases from the literature. Autoimmun Rev 2016; 15(12): 1129–1133. - PubMed
-
- Brain L, Jellinek EH, Ball K. Hashimoto’s disease and encephalopathy. Lancet 1966; 2(7462): 512–514. - PubMed
-
- Aydin-Ozemir Z, Tuzun E, Baykan B, et al. Autoimmune thyroid encephalopathy presenting with epilepsia partialis continua. Clin EEG Neurosci 2006; 37(3): 204–209. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
