

Determination of Eligibility for Influenza Research: A Clinical Informatics Approach
- PMID: 31205975
- PMCID: PMC6557306
- DOI: 10.1093/ofid/ofz231
Determination of Eligibility for Influenza Research: A Clinical Informatics Approach
Abstract
Background: A clinical informatics algorithm (CIA) was developed to systematically identify potential enrollees for a test-negative, case-control study to determine influenza vaccine effectiveness, to improve enrollment over manual records review. Further testing may enhance the CIA for increased efficiency.
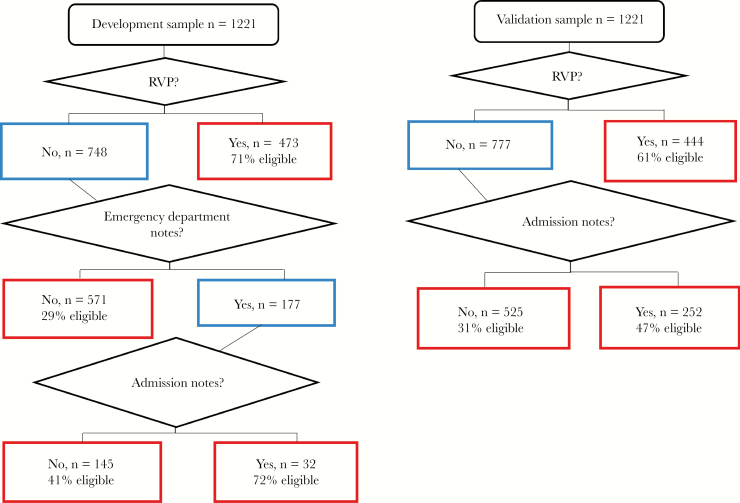
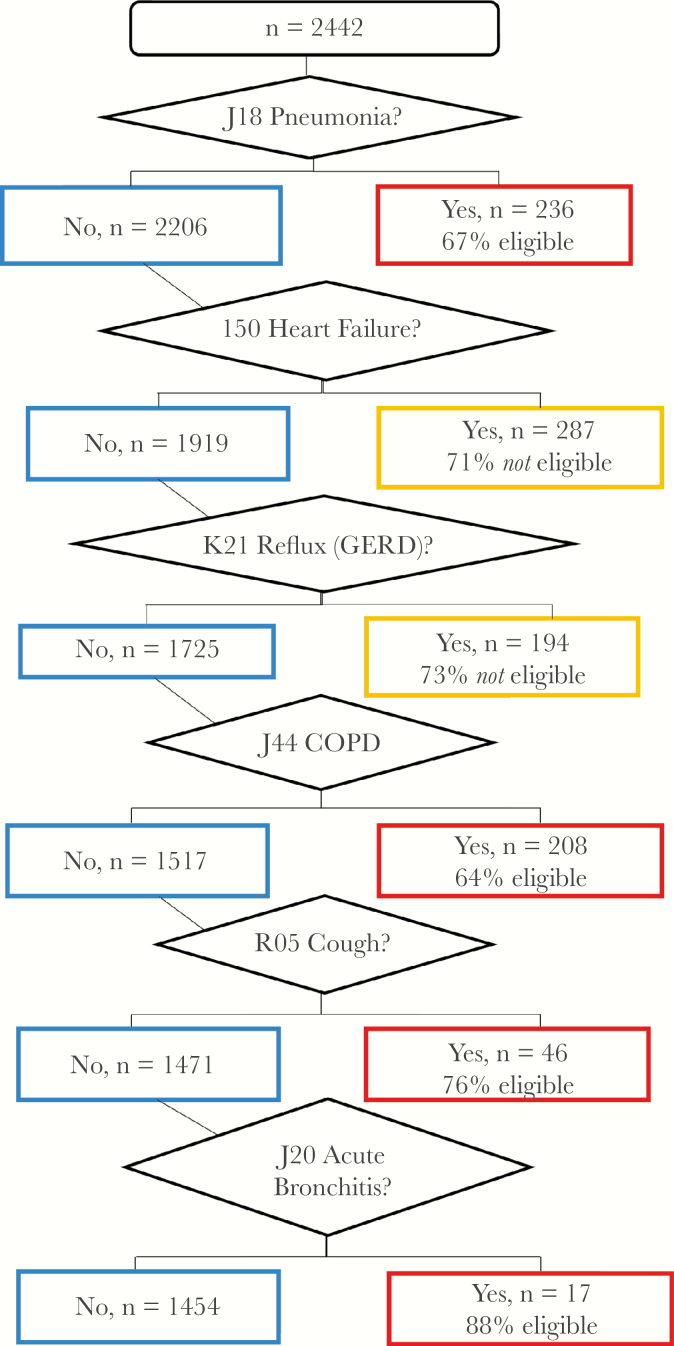
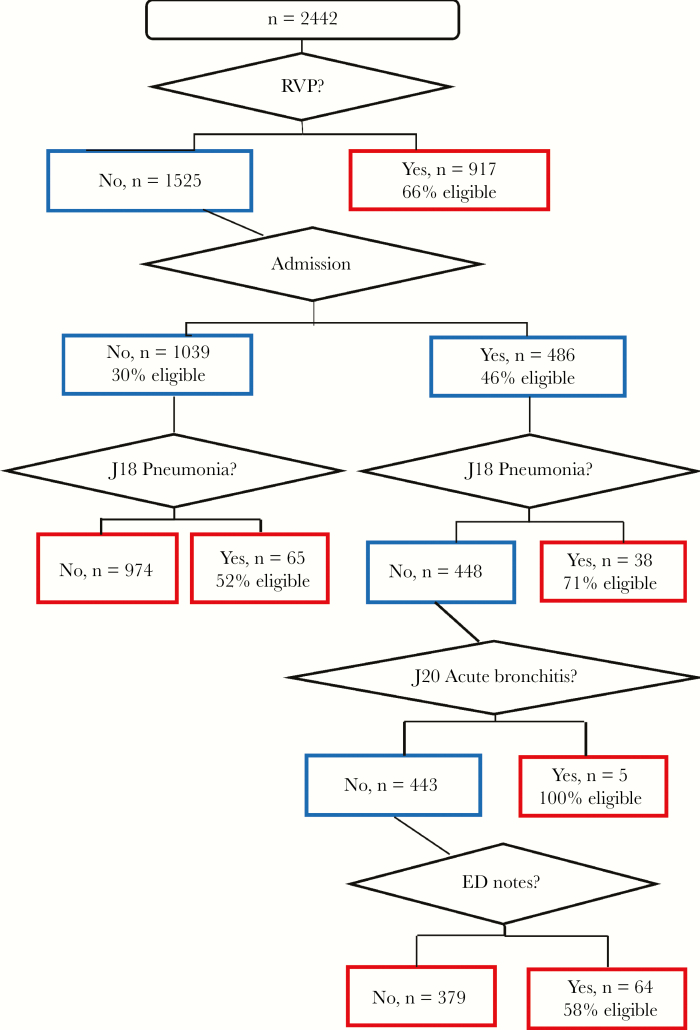
Methods: The CIA generated a daily screening list by querying all medical record databases for patients admitted in the last 3 days, using specified terms and diagnosis codes located in admission notes, emergency department notes, chief complaint upon registration, or presence of a respiratory viral panel charge or laboratory result (RVP). Classification and regression tree analysis (CART) and multivariable logistic regression were used to refine the algorithm.
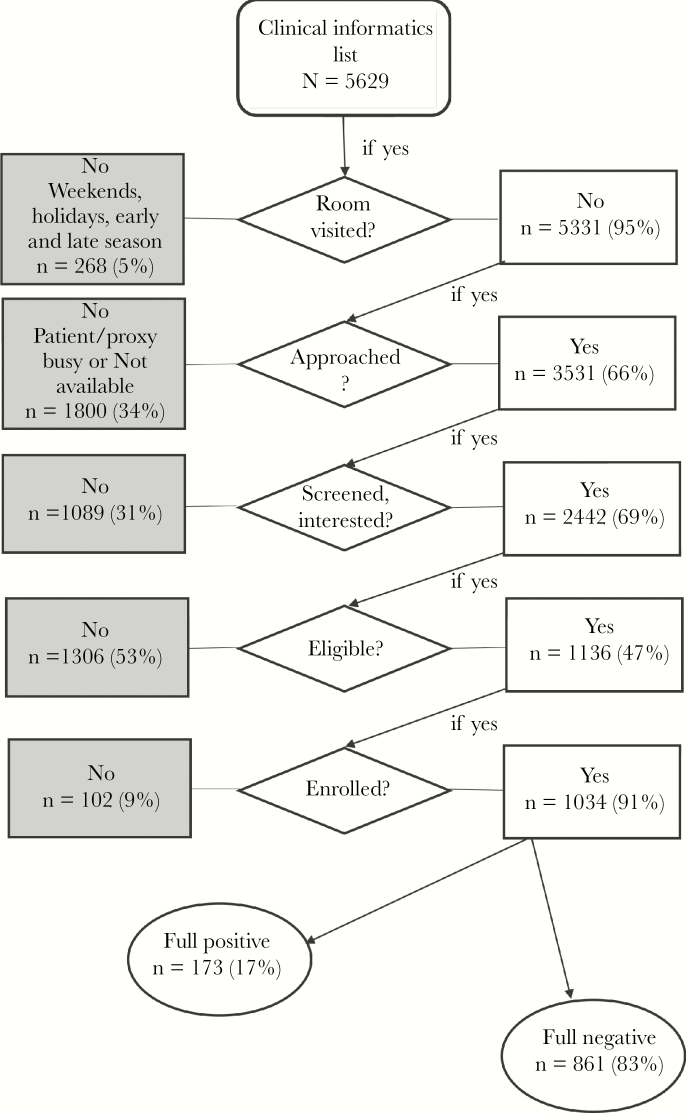
Results: Using manual records review, 204 patients (<4/day) were approached and 144 were eligible in the 2014-2015 season compared with 3531 (12/day) patients who were approached and 1136 who were eligible in the 2016-2017 season using a CIA. CART analysis identified RVP as the most important indicator from the CIA list for determining eligibility, identifying 65%-69% of the samples and predicting 1587 eligible patients. RVP was confirmed as the most significant predictor in regression analysis, with an odds ratio (OR) of 4.9 (95% confidence interval [CI], 4.0-6.0). Other significant factors were indicators in admission notes (OR, 2.3 [95% CI, 1.9-2.8]) and emergency department notes (OR, 1.8 [95% CI, 1.4-2.3]).
Conclusions: This study supports the benefits of a CIA to facilitate recruitment of eligible participants in clinical research over manual records review. Logistic regression and CART identified potential eligibility screening criteria reductions to improve the CIA's efficiency.
Keywords: acute respiratory infection; influenza vaccination; respiratory viral panel.
Figures
Similar articles
-
Efficacy and cost-effectiveness of an automated screening algorithm in an inpatient clinical trial.Clin Trials. 2012 Apr;9(2):198-203. doi: 10.1177/1740774511434844. Epub 2012 Feb 3. Clin Trials. 2012. PMID: 22308560 Free PMC article.
-
Association of Prior Vaccination With Influenza Vaccine Effectiveness in Children Receiving Live Attenuated or Inactivated Vaccine.JAMA Netw Open. 2018 Oct 5;1(6):e183742. doi: 10.1001/jamanetworkopen.2018.3742. JAMA Netw Open. 2018. PMID: 30646262 Free PMC article.
-
Potential Utility of Multiplex Amplification Respiratory Viral Panel Testing in the Management of Acute Respiratory Infection in Children: A Retrospective Analysis.J Pediatric Infect Dis Soc. 2014 Jun;3(2):146-53. doi: 10.1093/jpids/pit073. Epub 2013 Nov 13. J Pediatric Infect Dis Soc. 2014. PMID: 26625367
-
Systematic reviews of the effectiveness of day care for people with severe mental disorders: (1) acute day hospital versus admission; (2) vocational rehabilitation; (3) day hospital versus outpatient care.Health Technol Assess. 2001;5(21):1-75. doi: 10.3310/hta5210. Health Technol Assess. 2001. PMID: 11532238 Review.
-
Duration of Influenza Vaccine Effectiveness: A Systematic Review, Meta-analysis, and Meta-regression of Test-Negative Design Case-Control Studies.J Infect Dis. 2018 Feb 14;217(5):731-741. doi: 10.1093/infdis/jix632. J Infect Dis. 2018. PMID: 29220496
References
-
- Fiore AE, Bridges CB, Katz JM, Cox NJ. Inactivated influenza vaccines. In: Plotkin S, Orenstein W, Offit P, eds. Vaccines. 6th ed Philadelphia, PA: Elsevier Saunders; 2013:257–93.
-
- Estabragh ZR, Mamas MA. The cardiovascular manifestations of influenza: a systematic review. Int J Cardiol 2013; 167:2397–403. - PubMed
-
- Nichol KL, Wuorenma J, von Sternberg T. Benefits of influenza vaccination for low-, intermediate-, and high-risk senior citizens. Arch Intern Med 1998; 158:1769–76. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
