

Association of Elevated Plasma Interleukin-18 Level With Increased Mortality in a Clinical Trial of Statin Treatment for Acute Respiratory Distress Syndrome
- PMID: 31206358
- PMCID: PMC6629502
- DOI: 10.1097/CCM.0000000000003816
Association of Elevated Plasma Interleukin-18 Level With Increased Mortality in a Clinical Trial of Statin Treatment for Acute Respiratory Distress Syndrome
Abstract
Objective: A high plasma level of inflammasome mediator interleukin-18 was associated with mortality in observational acute respiratory distress syndrome cohorts. Statin exposure increases both inflammasome activation and lung injury in mouse models. We tested whether randomization to statin therapy correlated with increased interleukin-18 in the ARDS Network Statins for Acutely Injured Lungs from Sepsis trial.
Design: Retrospective analysis of randomized controlled clinical trial.
Setting: Multicenter North American clinical trial, the ARDS Network Statins for Acutely Injured Lungs from Sepsis.
Patients: Six hundred eighty-three subjects with infection-related acute respiratory distress syndrome, representing 92% of the original trial population.
Interventions: Random assignment of rosuvastatin or placebo for up to 28 days or 3 days after ICU discharge.
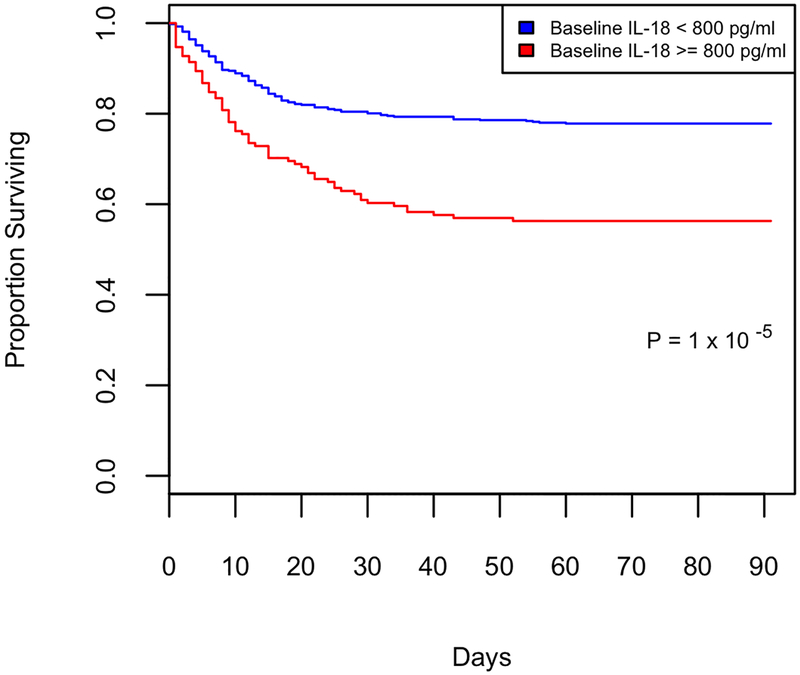
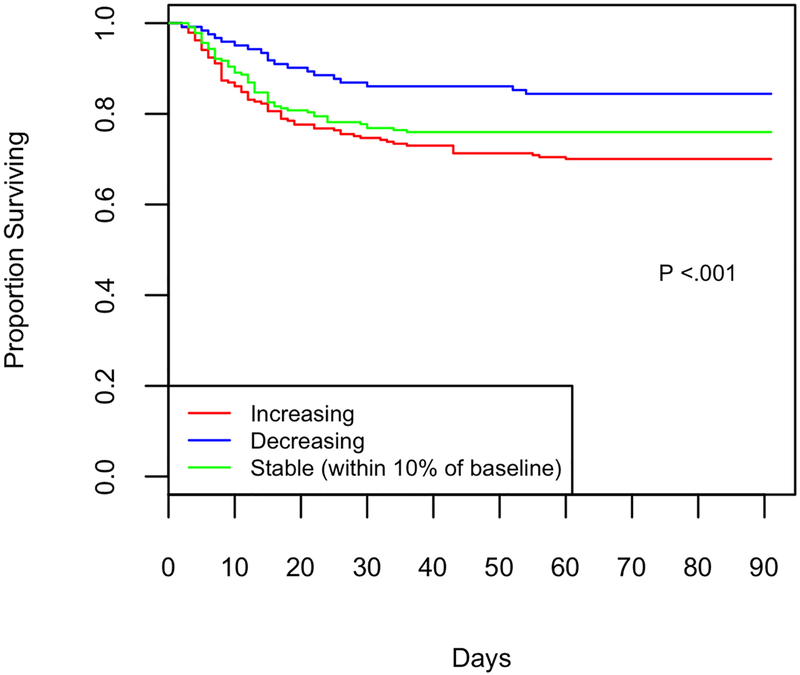
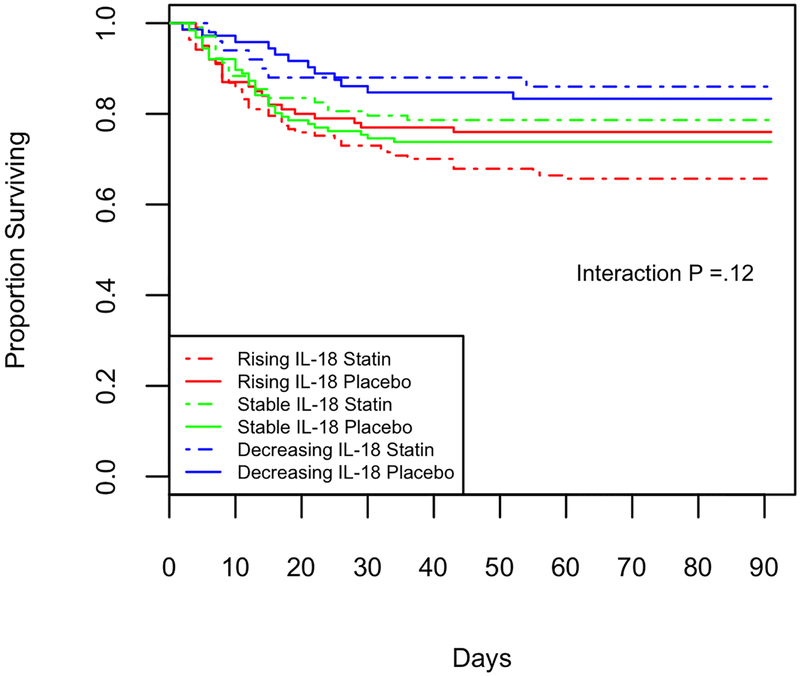
Measurements and main results: We measured plasma interleukin-18 levels in all Statins for Acutely Injured Lungs from Sepsis patients with sample available at day 0 (baseline, n = 683) and day 3 (after randomization, n = 588). We tested the association among interleukin-18 level at baseline, rising interleukin-18, and the impact of statin therapy on 60-day mortality, adjusting for severity of illness. Baseline plasma interleukin-18 level greater than or equal to 800 pg/mL was highly associated with 60-day mortality, with a hazard of death of 2.3 (95% CI, 1.7-3.1). Rising plasma interleukin-18 was also associated with increased mortality. For each unit increase in log2 (interleukin-18) at day 3 compared with baseline, the hazard of death increased by 2.3 (95% CI, 1.5-3.5). Subjects randomized to statin were significantly more likely to experience a rise in plasma interleukin-18 levels. Subjects with acute kidney injury, shock, low baseline interleukin-18, and those not receiving systemic corticosteroids were more likely to experience rising interleukin-18. Randomization to statin therapy was associated with rising in interleukin-18 in all of those subsets, however.
Conclusions: Elevated baseline plasma interleukin-18 was associated with higher mortality in sepsis-induced acute respiratory distress syndrome. A rise in plasma interleukin-18 was also associated with increased mortality and was more common in subjects randomized to statin therapy in this clinical trial.
Figures
Comment in
-
Inflammasomes Assemble: Cytoplasmic Guardians or Fallen Heroes?Crit Care Med. 2019 Aug;47(8):1161-1163. doi: 10.1097/CCM.0000000000003872. Crit Care Med. 2019. PMID: 31305304 Free PMC article. No abstract available.
-
Causal Inference With Mediation Analysis.Crit Care Med. 2020 Jan;48(1):e77-e78. doi: 10.1097/CCM.0000000000003998. Crit Care Med. 2020. PMID: 31833990 No abstract available.
-
The authors reply.Crit Care Med. 2020 Jan;48(1):e78. doi: 10.1097/CCM.0000000000004081. Crit Care Med. 2020. PMID: 31833991 No abstract available.
-
Are certain drugs associated with enhanced mortality in COVID-19?QJM. 2020 Jul 1;113(7):509-510. doi: 10.1093/qjmed/hcaa103. QJM. 2020. PMID: 32219440 Free PMC article. No abstract available.
References
-
- Chalmers JD, Singanayagam A, Murray MP, et al. Prior statin use is associated with improved outcomes in community-acquired pneumonia. Am J Med 2008;121(11):1002–1007 e1001. - PubMed
-
- Thomsen RW, Riis A, Kornum JB, et al. Preadmission use of statins and outcomes after hospitalization with pneumonia: population-based cohort study of 29,900 patients. Archives of internal medicine 2008;168(19):2081–2087. - PubMed
-
- Terblanche M, Almog Y, Rosenson RS, et al. Statins: panacea for sepsis? The Lancet Infectious diseases 2006;6(4):242–248. - PubMed
-
- Craig TR, Duffy MJ, Shyamsundar M, et al. A randomized clinical trial of hydroxymethylglutaryl- coenzyme a reductase inhibition for acute lung injury (The HARP Study). Am J Respir Crit Care Med 2011;183(5):620–626. - PubMed
