

The fetal origins of mental illness
- PMID: 31207234
- PMCID: PMC6889013
- DOI: 10.1016/j.ajog.2019.06.013
The fetal origins of mental illness
Abstract
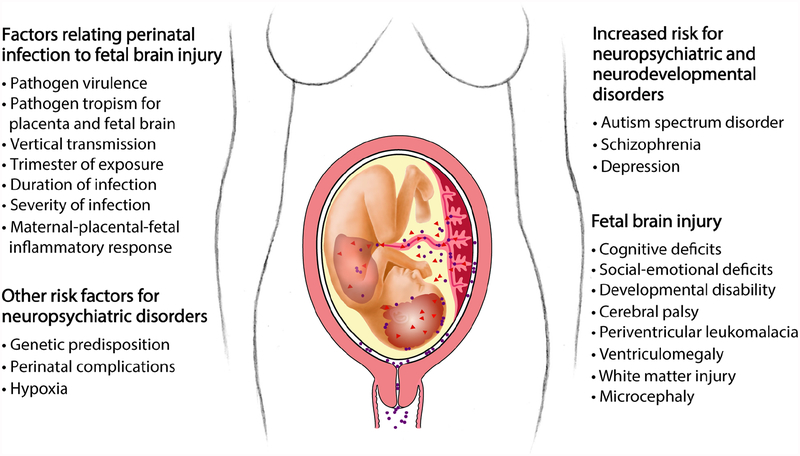
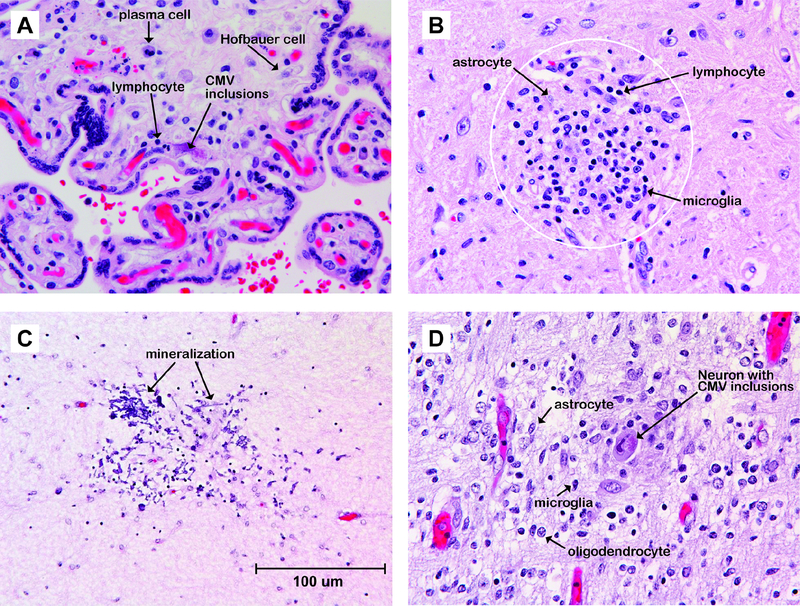
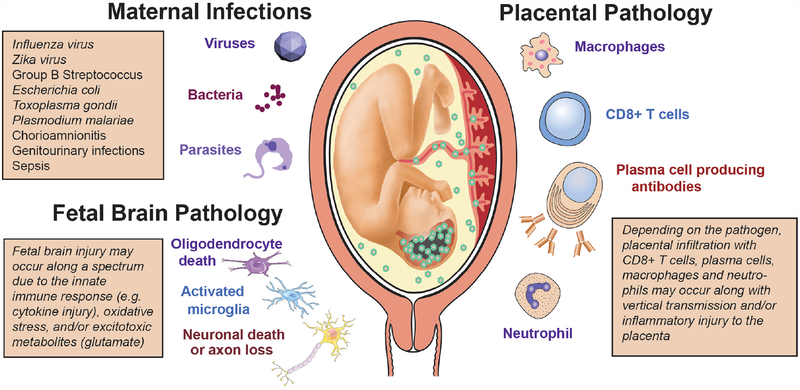
The impact of infections and inflammation during pregnancy on the developing fetal brain remains incompletely defined, with important clinical and research gaps. Although the classic infectious TORCH pathogens (ie, Toxoplasma gondii, rubella virus, cytomegalovirus [CMV], herpes simplex virus) are known to be directly teratogenic, emerging evidence suggests that these infections represent the most extreme end of a much larger spectrum of injury. We present the accumulating evidence that prenatal exposure to a wide variety of viral and bacterial infections-or simply inflammation-may subtly alter fetal brain development, leading to neuropsychiatric consequences for the child later in life. The link between influenza infections in pregnant women and an increased risk for development of schizophrenia in their children was first described more than 30 years ago. Since then, evidence suggests that a range of infections during pregnancy may also increase risk for autism spectrum disorder and depression in the child. Subsequent studies in animal models demonstrated that both pregnancy infections and inflammation can result in direct injury to neurons and neural progenitor cells or indirect injury through activation of microglia and astrocytes, which can trigger cytokine production and oxidative stress. Infectious exposures can also alter placental serotonin production, which can perturb neurotransmitter signaling in the developing brain. Clinically, detection of these subtle injuries to the fetal brain is difficult. As the neuropsychiatric impact of perinatal infections or inflammation may not be known for decades after birth, our construct for defining teratogenic infections in pregnancy (eg, TORCH) based on congenital anomalies is insufficient to capture the full adverse impact on the child. We discuss the clinical implications of this body of evidence and how we might place greater emphasis on prevention of prenatal infections. For example, increasing uptake of the seasonal influenza vaccine is a key strategy to reduce perinatal infections and the risk for fetal brain injury. An important research gap exists in understanding how antibiotic therapy during pregnancy affects the fetal inflammatory load and how to avoid inflammation-mediated injury to the fetal brain. In summary, we discuss the current evidence and mechanisms linking infections and inflammation with the increased lifelong risk of neuropsychiatric disorders in the child, and how we might improve prenatal care to protect the fetal brain.
Keywords: TORCH; autism; brain; depression; fetus; infection; inflammation; influenza virus; microglia; neuronal injury; pregnancy; schizophrenia; seasonality of birth hypothesis; urinary tract infection.
Copyright © 2019 Elsevier Inc. All rights reserved.
Conflict of interest statement
The authors report no conflict of interest.
Figures
Comment in
-
Antibiotics, pregnancy, and fetal mental illnesses: where is the link?Am J Obstet Gynecol. 2020 Jun;222(6):639-640. doi: 10.1016/j.ajog.2020.01.050. Epub 2020 Feb 1. Am J Obstet Gynecol. 2020. PMID: 32017921 No abstract available.
-
Reply.Am J Obstet Gynecol. 2020 Aug;223(2):301-302. doi: 10.1016/j.ajog.2020.03.014. Epub 2020 Mar 14. Am J Obstet Gynecol. 2020. PMID: 32184146 No abstract available.
-
Other causes of fetal brain injury.Am J Obstet Gynecol. 2020 Aug;223(2):301. doi: 10.1016/j.ajog.2020.03.013. Epub 2020 Mar 14. Am J Obstet Gynecol. 2020. PMID: 32184152 No abstract available.
References
-
- Parisot S, Droulle P, Feldmann M, Pinaud P, Marchal C. Unusual encephaloclastic lesions with paraventricular calcification in congenital rubella. Pediatr Radiol. 1991;21(3):229–230. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
