

The accuracy of ischemic core perfusion thresholds varies according to time to recanalization in stroke patients treated with mechanical thrombectomy: A comprehensive whole-brain computed tomography perfusion study
- PMID: 31208242
- PMCID: PMC7181085
- DOI: 10.1177/0271678X19855885
The accuracy of ischemic core perfusion thresholds varies according to time to recanalization in stroke patients treated with mechanical thrombectomy: A comprehensive whole-brain computed tomography perfusion study
Abstract
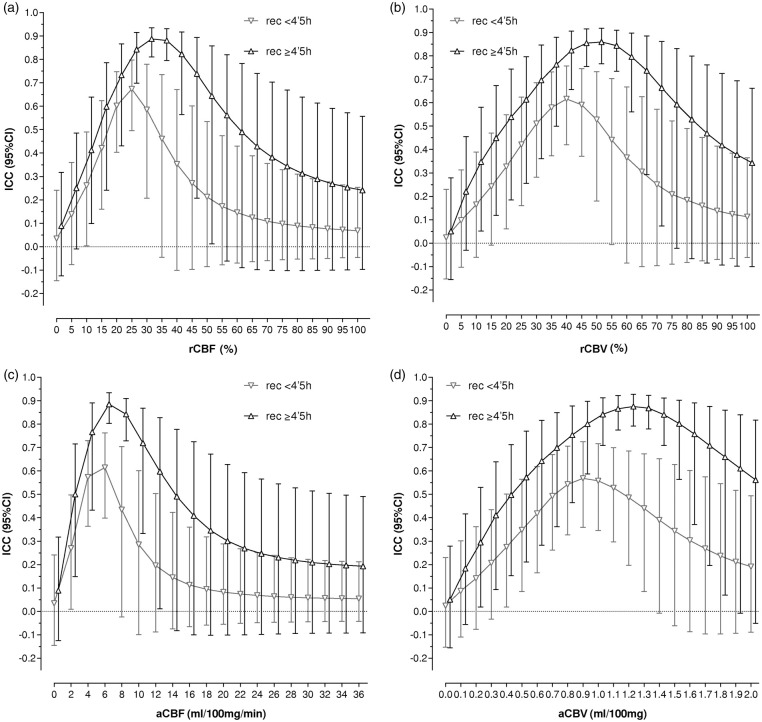
Computed tomography perfusion (CTP) allows the estimation of pretreatment ischemic core after acute ischemic stroke. However, CTP-derived ischemic core may overestimate final infarct volume. We aimed to evaluate the accuracy of CTP-derived ischemic core for the prediction of final infarct volume according to time from stroke onset to recanalization in 104 patients achieving complete recanalization after mechanical thrombectomy who had a pretreatment CTP and a 24-h follow-up MRI-DWI. A range of CTP thresholds was explored in perfusion maps at constant increments for ischemic core calculation. Time to recanalization modified significantly the association between ischemic core and DWI lesion in a non-linear fashion (p-interaction = 0.018). Patients with recanalization before 4.5 h had significantly lower intraclass correlation coefficient (ICC) values between CTP-predicted ischemic core and DWI lesion (n = 54; best threshold relative cerebral blood flow (rCBF) < 25%, ICC = 0.673, 95% CI = 0.495-0.797) than those with later recanalization (n = 50; best threshold rCBF < 30%, ICC = 0.887, 95% CI = 0.811-0.935, p = 0.013), as well as poorer spatial lesion agreement. The significance of the associations between CTP-derived ischemic core and clinical outcome at 90 days was lost in patients recanalized before 4.5 h. CTP-derived ischemic core must be interpreted with caution given its dependency on time to recanalization, primarily in patients with higher chances of early recanalization.
Keywords: Computed tomography perfusion; ischemic core; ischemic stroke; recanalization; thrombectomy.
Figures




Similar articles
-
Predictors of ghost infarct core on baseline computed tomography perfusion in stroke patients with successful recanalization after mechanical thrombectomy.Eur Radiol. 2023 Mar;33(3):1792-1800. doi: 10.1007/s00330-022-09189-1. Epub 2022 Oct 25. Eur Radiol. 2023. PMID: 36282310
-
Spatial accuracy of computed tomography perfusion to estimate the follow-up infarct on diffusion-weighted imaging after successful mechanical thrombectomy.BMC Neurol. 2023 Jan 20;23(1):31. doi: 10.1186/s12883-023-03075-z. BMC Neurol. 2023. PMID: 36670367 Free PMC article.
-
Pretreatment brain CT perfusion thresholds for predicting final infarct volume in distal medium vessel occlusions.J Neuroimaging. 2023 Nov-Dec;33(6):968-975. doi: 10.1111/jon.13142. Epub 2023 Jun 25. J Neuroimaging. 2023. PMID: 37357133
-
Automated CT Perfusion Detection of the Acute Infarct Core in Ischemic Stroke: A Systematic Review and Meta-Analysis.Cerebrovasc Dis. 2023;52(1):97-109. doi: 10.1159/000524916. Epub 2022 Jun 3. Cerebrovasc Dis. 2023. PMID: 35661075
-
Reperfusion Injury Is Associated With Poor Outcome in Patients With Recanalization After Thrombectomy.Stroke. 2023 Jan;54(1):96-104. doi: 10.1161/STROKEAHA.122.039337. Epub 2022 Nov 11. Stroke. 2023. PMID: 36367100 Review.
Cited by
-
Deep learning-based identification of acute ischemic core and deficit from non-contrast CT and CTA.J Cereb Blood Flow Metab. 2021 Nov;41(11):3028-3038. doi: 10.1177/0271678X211023660. Epub 2021 Jun 8. J Cereb Blood Flow Metab. 2021. PMID: 34102912 Free PMC article.
-
CT Perfusion as a Predictor of the Final Infarct Volume in Patients with Tandem Occlusion.J Pers Med. 2023 Feb 16;13(2):342. doi: 10.3390/jpm13020342. J Pers Med. 2023. PMID: 36836576 Free PMC article.
-
Accuracy of CT Perfusion-Based Core Estimation of Follow-up Infarction: Effects of Time Since Last Known Well.Neurology. 2022 May 24;98(21):e2084-e2096. doi: 10.1212/WNL.0000000000200269. Epub 2022 Apr 21. Neurology. 2022. PMID: 35450966 Free PMC article.
-
Leukoaraiosis May Confound the Interpretation of CT Perfusion in Patients Treated with Mechanical Thrombectomy for Acute Ischemic Stroke.AJNR Am J Neuroradiol. 2019 Aug;40(8):1323-1329. doi: 10.3174/ajnr.A6139. Epub 2019 Jul 25. AJNR Am J Neuroradiol. 2019. PMID: 31345941 Free PMC article.
-
Neurological Functional Independence After Endovascular Thrombectomy and Different Imaging Modalities for Large Infarct Core Assessment : A Systematic Review and Meta-analysis.Clin Neuroradiol. 2023 Mar;33(1):21-29. doi: 10.1007/s00062-022-01202-w. Epub 2022 Aug 3. Clin Neuroradiol. 2023. PMID: 35920865
References
-
- Lev MH. Perfusion imaging of acute stroke: its role in current and future clinical practice. Radiology 2013; 266: 22–27. - PubMed
-
- Campbell BCV, Christensen SS, Levi CR, et al.Cerebral blood flow is the optimal CT perfusion parameter for assessing infarct core. Stroke 2011; 42: 3435–3440. - PubMed
-
- Campbell BCV, Christensen SS, Levi CR, et al.Comparison of computed tomography perfusion and magnetic resonance imaging perfusion-diffusion mismatch in ischemic stroke. Stroke 2012; 43: 2648–53. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
