

Vitamin D deficiency is associated with risk of developing peripheral arterial disease in type 2 diabetic patients
- PMID: 31208330
- PMCID: PMC6580529
- DOI: 10.1186/s12872-019-1125-0
Vitamin D deficiency is associated with risk of developing peripheral arterial disease in type 2 diabetic patients
Abstract
Background: The relationship between vitamin D levels and peripheral arterial disease (PAD) remains unclear. We assessed the association of serum 25-hydroxyvitamin D (25(OH)D) levels with the prevalence of PAD in patients with type 2 diabetes mellitus(T2DM).
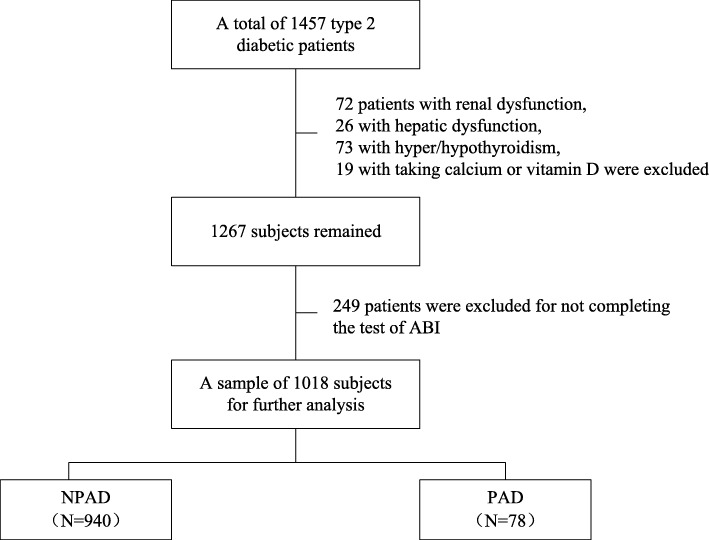
Methods: A total of 1018 T2DM patients participated in this cross-sectional study. Serum 25(OH)D levels were measured and risk factors of PAD were recorded. PAD was diagnosed as an ankle-brachial index (ABI) < 0.9.
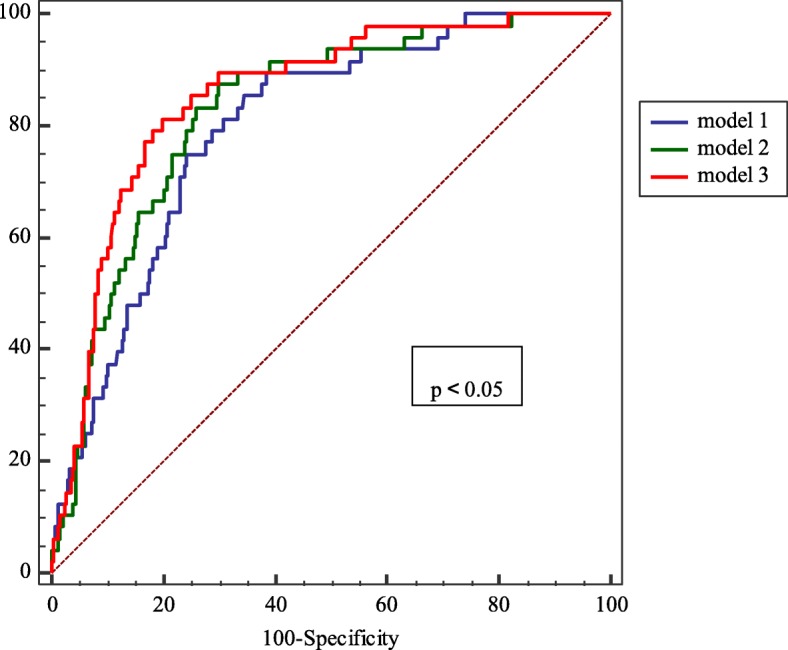
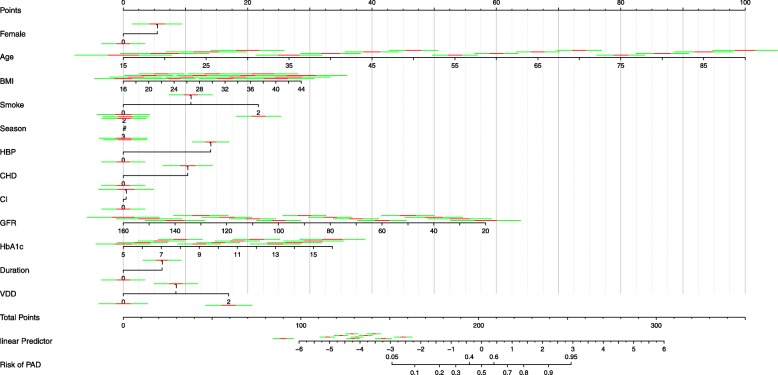
Results: The mean age of the diabetic patients was 58.59 ± 11.34 years. Of all the patients, only 20.1% had a 25(OH)D level ≥ 20 ng/mL. Compared to patients without PAD, serum 25(OH)D levels were significantly lower in those with PAD (14.81 ± 8.43 vs. 11.55 ± 5.65 ng/mL, P < 0.001). The overall prevalence of PAD was 7.7%. From the highest level (≥ 20 ng/mL) to the lowest level (< 10 ng/mL) of serum 25(OH)D, the prevalence of PAD was 2.8, 7.5 and 10.7% respectively. After adjustment for age, sex, body mass index (BMI), smoking status and season, compared to patients with serum 25(OH)D levels ≥20 ng/mL, the odds ratios of PAD in patients with a level of 10 to < 20 ng/mL and < 10 ng/mL was 3.587(95% CI: 1.314-9.790) and 5.540(95% CI: 2.004-15.320), respectively. When further considering the influence of coronary heart disease (CHD), hypertension and cerebral infarction, the ratios changed to 3.824(95% CI: 1.378-10.615) and 5.729(95% CI: 2.028-16.187), respectively. And after further adjustment for the duration of diabetes, glycated hemoglobin (HbA1c) and glomerular filtration rate (GFR), the ratios changed to 3.489(95% CI: 1.100-11.062) and 3.872(95% CI: 1.168-12.841), respectively.
Conclusions: Reduced serum vitamin D levels were associated with an increased risk of PAD in T2DM patients. Randomized interventive clinical studies are required to verify the effects of vitamin D supplementation on PAD.
Keywords: 25-hydroxyvitamin D; Peripheral arterial disease; Type 2 diabetes; Vitamin D deficiency.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Vitamin D Deficiency May Not Be an Independent Risk Factor for Peripheral Arterial Disease in Middle-Aged and Elderly Patients with Type 2 Diabetes in China.Dis Markers. 2020 Nov 25;2020:8854717. doi: 10.1155/2020/8854717. eCollection 2020. Dis Markers. 2020. PMID: 33299499 Free PMC article.
-
Low 25-Hydroxyvitamin D Level Is Associated with Peripheral Arterial Disease in Type 2 Diabetes Patients.Arch Med Res. 2016 Jan;47(1):49-54. doi: 10.1016/j.arcmed.2016.01.007. Epub 2016 Feb 6. Arch Med Res. 2016. PMID: 26854799
-
Correlation Analysis between Serum Vitamin D Levels and Lower Extremity Macrovascular Complications in Individuals with Type 2 Diabetes Mellitus.J Diabetes Res. 2019 Nov 28;2019:4251829. doi: 10.1155/2019/4251829. eCollection 2019. J Diabetes Res. 2019. PMID: 31871946 Free PMC article.
-
The association of circulating 25-hydroxyvitamin D concentration with peripheral arterial disease: A meta-analysis of observational studies.Atherosclerosis. 2015 Dec;243(2):645-51. doi: 10.1016/j.atherosclerosis.2015.10.011. Epub 2015 Oct 14. Atherosclerosis. 2015. PMID: 26554715 Review.
-
Body Mass Index, Vitamin D, and Type 2 Diabetes: A Systematic Review and Meta-Analysis.Nutrients. 2018 Aug 28;10(9):1182. doi: 10.3390/nu10091182. Nutrients. 2018. PMID: 30154381 Free PMC article.
Cited by
-
Plasma Lipidomic Profiles Improve upon Traditional Risk Factors for the Prediction of Arterial Stiffness Among Patients with Type 2 Diabetes Mellitum: A Randomized, Placebo-Controlled Trial.Nutrients. 2024 Oct 25;16(21):3618. doi: 10.3390/nu16213618. Nutrients. 2024. PMID: 39519451 Free PMC article. Clinical Trial.
-
Vitamin D Deficiency May Not Be an Independent Risk Factor for Peripheral Arterial Disease in Middle-Aged and Elderly Patients with Type 2 Diabetes in China.Dis Markers. 2020 Nov 25;2020:8854717. doi: 10.1155/2020/8854717. eCollection 2020. Dis Markers. 2020. PMID: 33299499 Free PMC article.
-
Vitamin D: Not Just Bone Metabolism but a Key Player in Cardiovascular Diseases.Life (Basel). 2021 May 18;11(5):452. doi: 10.3390/life11050452. Life (Basel). 2021. PMID: 34070202 Free PMC article. Review.
-
Insulin Resistance and Vitamin D Deficiency: A Link Beyond the Appearances.Front Cardiovasc Med. 2022 Mar 17;9:859793. doi: 10.3389/fcvm.2022.859793. eCollection 2022. Front Cardiovasc Med. 2022. PMID: 35369303 Free PMC article. Review.
-
Could vitamin D deficiency influence left heart ventricular geometry in youngsters with type 1 diabetes mellitus?Hippokratia. 2019 Jan-Mar;23(1):9-14. Hippokratia. 2019. PMID: 32256032 Free PMC article.
References
-
- Kayaniyil S, Vieth R, Retnakaran R, Knight JA, Qi Y, Gerstein HC, Perkins BA, Harris SB, Zinman B, Hanley AJ. Association of vitamin D with insulin resistance and beta-cell dysfunction in subjects at risk for type 2 diabetes. Diabetes Care. 2010;33(6):1379–1381. doi: 10.2337/dc09-2321. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
