

Arrhythmic episodes in patients implanted with a cardioverter-defibrillator - results from the Prospective Study on Predictive Quality with Preferencing PainFree ATP therapies (4P)
- PMID: 31208342
- PMCID: PMC6580638
- DOI: 10.1186/s12872-019-1121-4
Arrhythmic episodes in patients implanted with a cardioverter-defibrillator - results from the Prospective Study on Predictive Quality with Preferencing PainFree ATP therapies (4P)
Abstract
Background: Little is known about the ICD performance using enhanced detection algorithms in unselected, non-trial patients. Performance of recent generation ICD equipped with SmartShock™ technology (SST) for detection and conversion of ventricular tachyarrhythmias (VTA) was investigated.
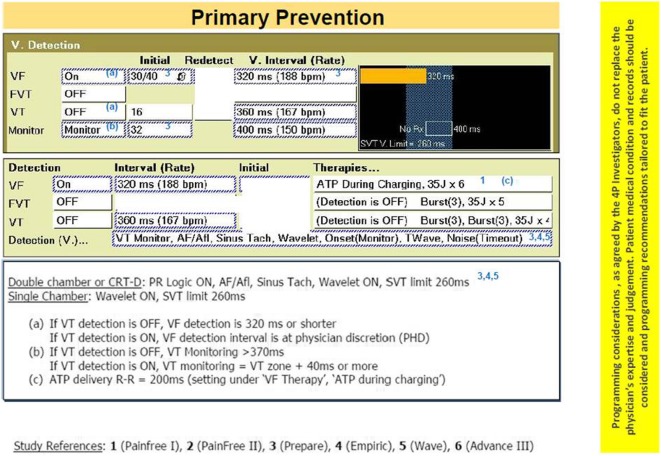
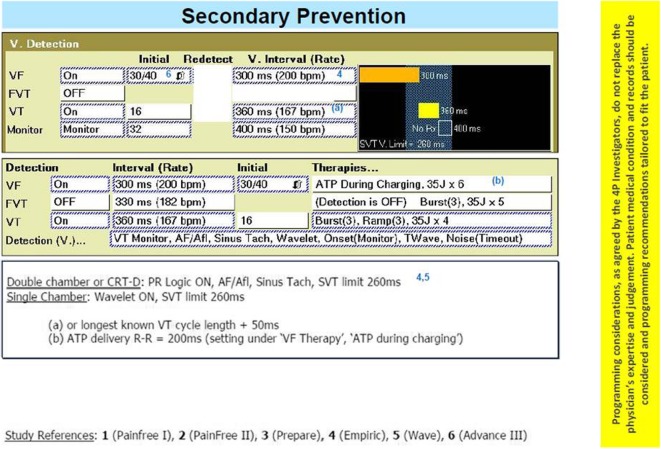
Methods: 4P was a prospective, multicenter, observational study conducted in 10 Swiss implanting centers. Patients with a Class I indication according to international guidelines were included and received an ICD with SST. ICD discrimination capability was assessed by evaluating SST performance; therapy efficacy was assessed by rate of VTA conversions by ATP and by rescue shocks.
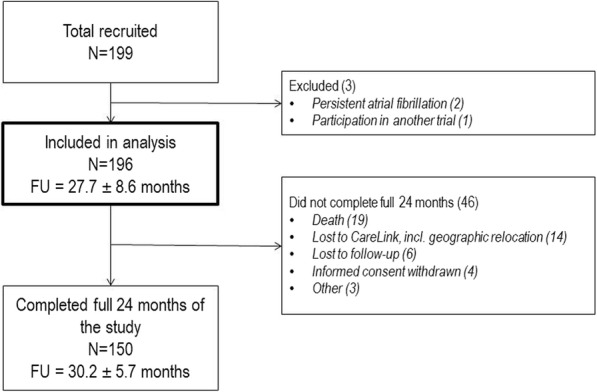
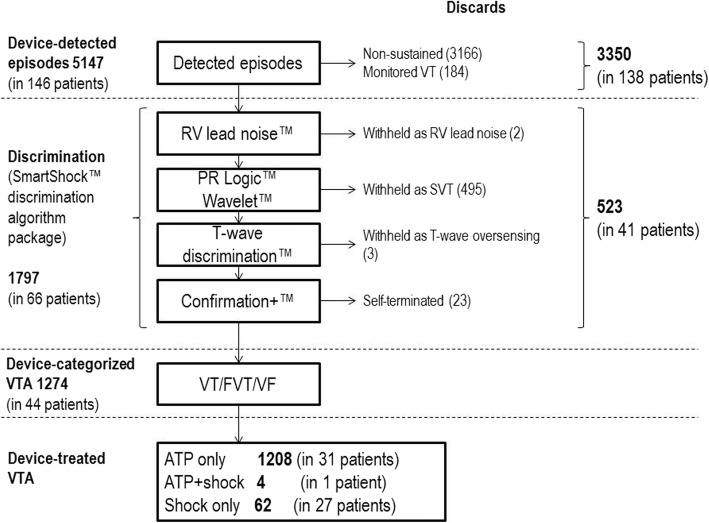
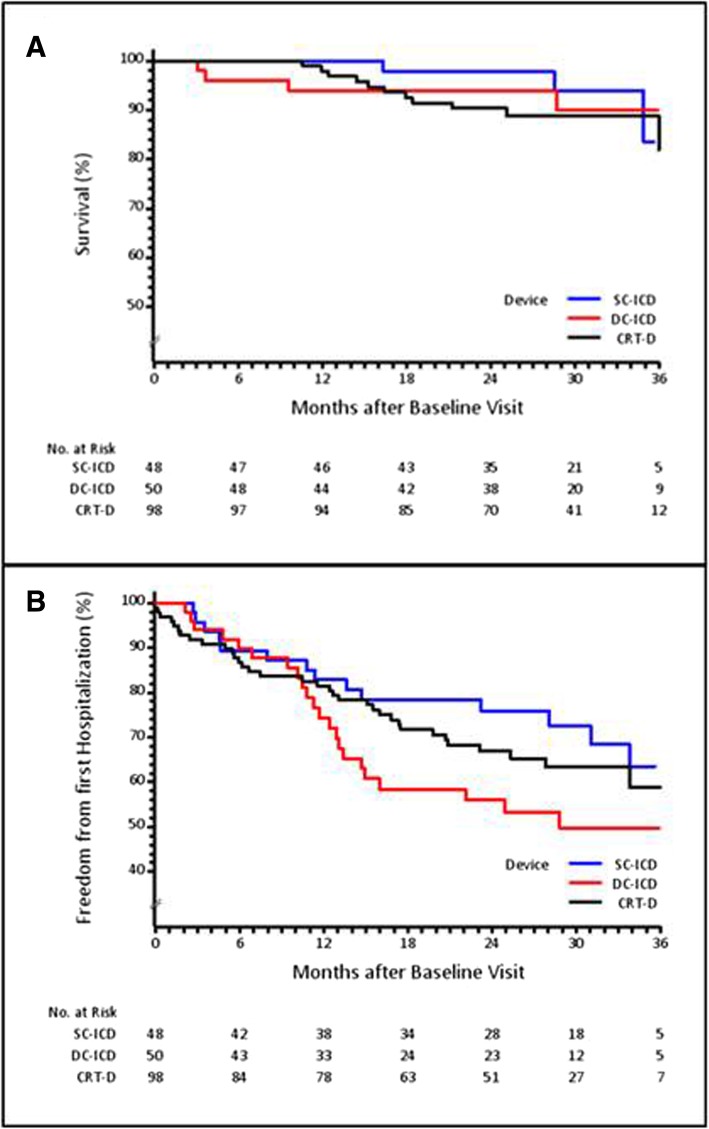
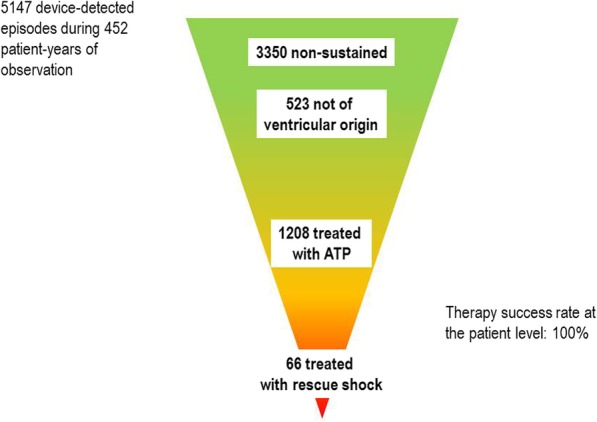
Results: Overall, 196 patients were included in the analysis with a mean duration of follow-up of 27.7 months (452 patient-years of observation). Patient-specific rather than recommended programming was preferred. Device-detected episodes were frequent (5147 episodes in 146 patients, 74.5%). In 44 patients (22.4%), 1274 episodes were categorized as VTA; only 215 episodes were symptomatic. ATP was the first-line therapy and highly effective (99.9% success rate at the episode level, 100.0% at the patient level). Rescue shocks were rare (66 episodes in 28 patients); 7 shocks in 5 patients (2.6%) were inappropriate. Death and hospitalization rates were low.
Conclusions: In a cohort of non-trial, unselected ICD patients, VTA episodes were frequent. The 4P results confirm the robustness of VTA detection by SST and the effectiveness of ATP treatment, hence limiting overall ICD shock burden.
Keywords: Antitachycardia pacing; Implantable cardioverter-defibrillator; Shock; Ventricular tachyarrhythmia.
Conflict of interest statement
Dr. François Regoli declares speaker and consultation fees from Bayer, Boston Scientific, Microport, Medtronic, and is associate editor for BMC Cardiovascular Disorders. Dr. Beat Schaer discloses speaker’s bureau fees from Medtronic and Microport. Dr. Peter Ammann is a European advisory board member for Medtronic. Lorenza Mangoni di S. Stefano is an employee of Medtronic Core Clinical Solutions. Dr. Martin Fromer is a consultant for Medtronic, Switzerland. Doctors Denis Graf, Firat Duru, Barbara Naegli, Haran Burri, Rainer Zbinden, Nazmi Krasniqi have no competing interests to declare.
Figures
Similar articles
-
Reprogramming the tachycardia parameters with long-detection strategy in patients with pre-existing implantable cardioverter-defibrillator.Acta Cardiol. 2019 Jun;74(3):246-251. doi: 10.1080/00015385.2018.1488664. Epub 2018 Jul 28. Acta Cardiol. 2019. PMID: 30058473
-
Prospective Randomized Evaluation of Implantable Cardioverter-Defibrillator Programming in Patients With a Left Ventricular Assist Device.J Am Heart Assoc. 2018 Feb 23;7(5):e007748. doi: 10.1161/JAHA.117.007748. J Am Heart Assoc. 2018. PMID: 29475875 Free PMC article. Clinical Trial.
-
SVT discrimination algorithms significantly reduce the rate of inappropriate therapy in the setting of modern-day delayed high-rate detection programming.J Cardiovasc Electrophysiol. 2019 Dec;30(12):2877-2884. doi: 10.1111/jce.14250. Epub 2019 Nov 5. J Cardiovasc Electrophysiol. 2019. PMID: 31646695
-
Recent developments in the subcutaneous ICD.Trends Cardiovasc Med. 2016 Aug;26(6):526-35. doi: 10.1016/j.tcm.2016.03.004. Epub 2016 Mar 15. Trends Cardiovasc Med. 2016. PMID: 27079889 Review.
-
The subcutaneous implantable cardioverter defibrillator in 2019 and beyond.Trends Cardiovasc Med. 2020 Aug;30(6):378-384. doi: 10.1016/j.tcm.2019.09.006. Epub 2019 Oct 1. Trends Cardiovasc Med. 2020. PMID: 31610949 Review.
Cited by
-
Assessing the Cost and Resource Use Impact of Implantable Cardiac Defibrillator Shocks in the UK CareLink Population.Clinicoecon Outcomes Res. 2023 Jun 6;15:425-432. doi: 10.2147/CEOR.S403712. eCollection 2023. Clinicoecon Outcomes Res. 2023. PMID: 37305155 Free PMC article.
-
Management of hemodynamically stable wide QRS complex tachycardia in patients with implantable cardioverter defibrillators.Front Cardiovasc Med. 2023 Jan 4;9:1011619. doi: 10.3389/fcvm.2022.1011619. eCollection 2022. Front Cardiovasc Med. 2023. PMID: 36684577 Free PMC article. Review.
References
-
- Wilkoff BL, Ousdigian KT, Sterns LD, Wang ZJ, Wilson RD, Morgan JM, et al. A comparison of empiric to physician-tailored programming of implantable cardioverter-defibrillators: results from the prospective randomized multicenter EMPIRIC trial. J Am Coll Cardiol. 2006;48:330–339. doi: 10.1016/j.jacc.2006.03.037. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
