

CO2 and O2 removal during continuous veno-venous hemofiltration: a pilot study
- PMID: 31208356
- PMCID: PMC6580471
- DOI: 10.1186/s12882-019-1378-y
CO2 and O2 removal during continuous veno-venous hemofiltration: a pilot study
Erratum in
-
Correction to: CO2 and O2 removal during continuous veno-venous hemofiltration: a pilot study.BMC Nephrol. 2019 Aug 8;20(1):312. doi: 10.1186/s12882-019-1480-1. BMC Nephrol. 2019. PMID: 31395021 Free PMC article.
Abstract
Background: Carbon dioxide (CO2) accumulation is a challenging issue in critically ill patients. CO2 can be eliminated by renal replacement therapy but studies are scarce and clinical relevance is unknown. We prospectively studied CO2 and O2 behavior at different sample points of continuous veno-venous hemofiltration (CVVH) and build a model to calculate CO2 removal bedside.
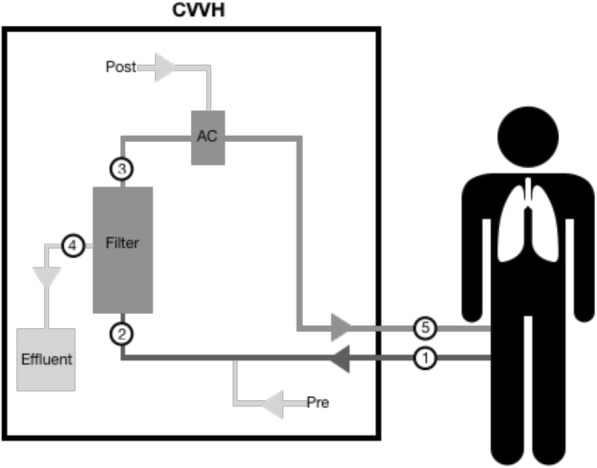
Methods: In 10 patients receiving standard CVVH under citrate anticoagulation, blood gas analysis was performed at different sample points within the CVVH circuit. Citrate was then replaced by NaCl 0.9% and sampling was repeated. Total CO2 (tCO2), CO2 flow (V̇CO2) and O2 flow (V̇O2) were compared between different sample points. The effect of citrate on transmembrane tCO2 was evaluated. Wilcoxon matched-pairs signed rank test was performed to evaluate significance of difference between 2 data sets. Friedman test was used when more data sets were compared.
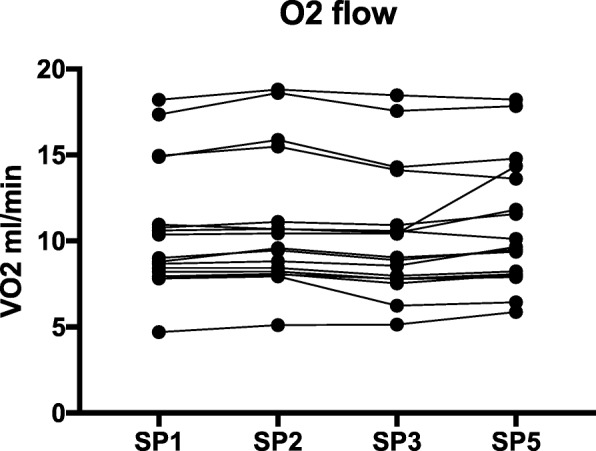
Results: V̇CO2 in the effluent (26.0 ml/min) correlated significantly with transmembrane V̇CO2 (24.2 ml/min). This represents 14% of the average expired V̇CO2 in ventilated patients. Only 1.3 ml/min CO2 was removed in the de-aeration chamber, suggesting that CO2 was almost entirely cleared across the membrane filter. tCO2 values in effluent, before, and after the filter were not statistically different. Transmembrane tCO2 under citrate or NaCl 0.9% predilution also did not differ significantly. No changes in V̇O2 were observed throughout the CVVH circuit. Based on recorded data, formulas were constructed that allow bedside evaluation of CVVH-attributable CO2 removal.
Conclusion: A relevant amount of CO2 is removed by CVVH and can be quantified by one simple blood gas analysis within the circuit. Future studies should assess the clinical impact of this observation.
Trial registration: The trial was registered at https://clinicaltrials.gov with trial registration number NCT03314363 on October 192,017.
Keywords: Carbon dioxide removal; Citrate; Continuous renal replacement therapy; Continuous veno-venous hemofiltration; Oxygen removal.
Conflict of interest statement
Dr. Jonckheer and Prof. Dr. De Waele have received a grant from Baxter as a replacement fee and for logistic support.
Figures





References
-
- Boron WF. Transport of oxygen and carbon dioxide in the blood. In: Boron WF, Boulpaep EL, editors. Medical physiology. 2005. pp. 654–668.
-
- Taccone FS, Malfertheiner MV, Ferrari F, et al. Extracorporeal CO2 removal in critically ill patients: a systematic review. Minerva Anestesiol. 2017;83(7):762–772. - PubMed
-
- Sherlock JE, Yoon Y, Ledwith JW, Letteri JM. Respiratory gas exchange during hemodialysis. Proc Clin Dial Transplant Forum. 1972;2:171–174. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
