

Conditional survival and changing risk profile in patients with chordoma: a population-based longitudinal cohort study
- PMID: 31208441
- PMCID: PMC6580628
- DOI: 10.1186/s13018-019-1225-7
Conditional survival and changing risk profile in patients with chordoma: a population-based longitudinal cohort study
Abstract
Objective: To evaluate the conditional survival of patients with chordoma to potentially help physician planning of optimal cancer surveillance and guide better clinical decisions.
Methods: In total, 1942 patients with chordoma were identified and extracted from Surveillance, Epidemiology, and End Results (SEER) databases (1973-2015). The cumulative survival estimates were used to calculate the conditional survival rate, and the Greenwood formula was used to estimate the 95% CI. In addition, multivariable Cox regression analyses were used to calculate hazard ratios, according to the duration of survival.
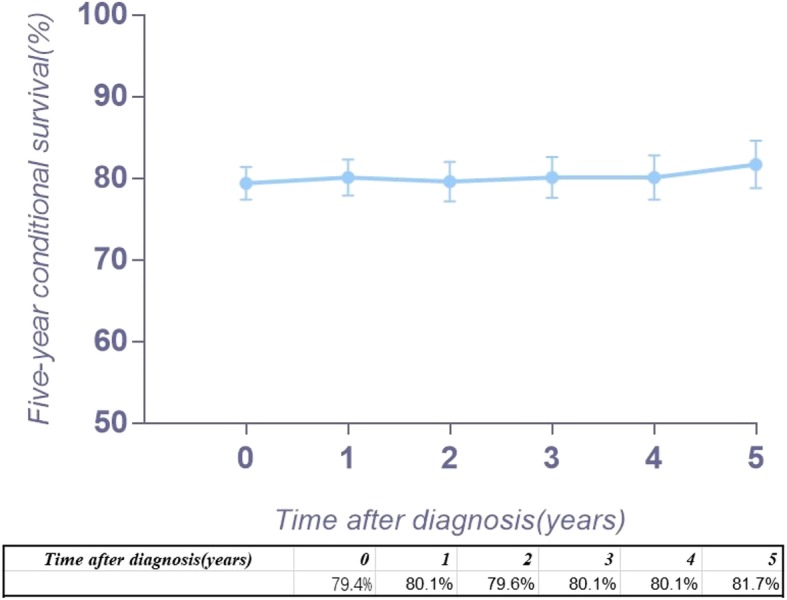
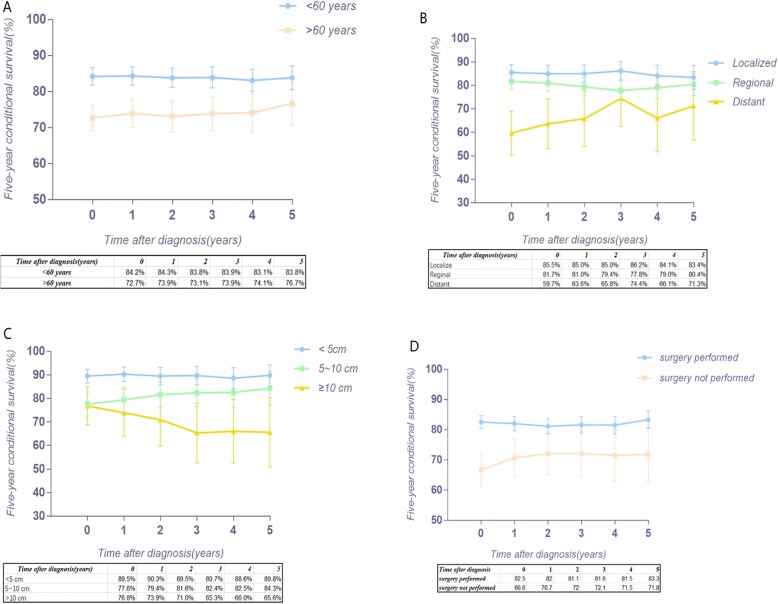
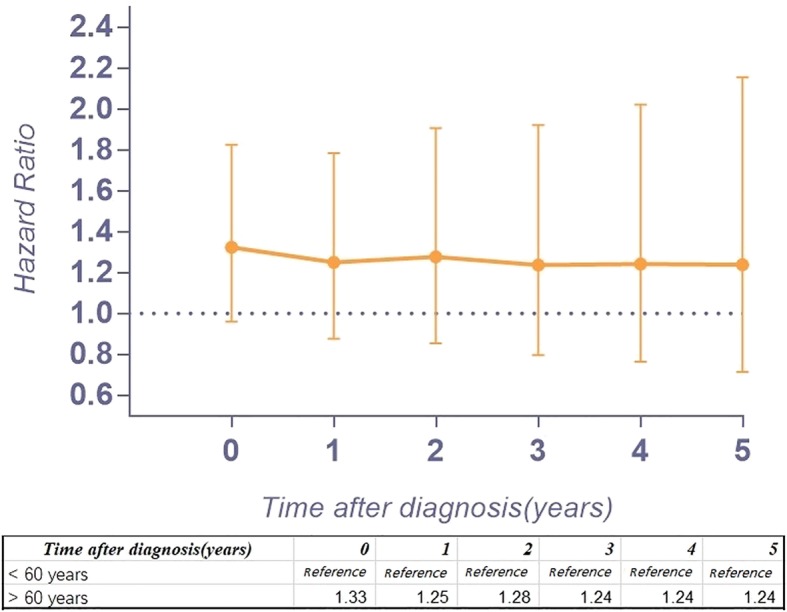
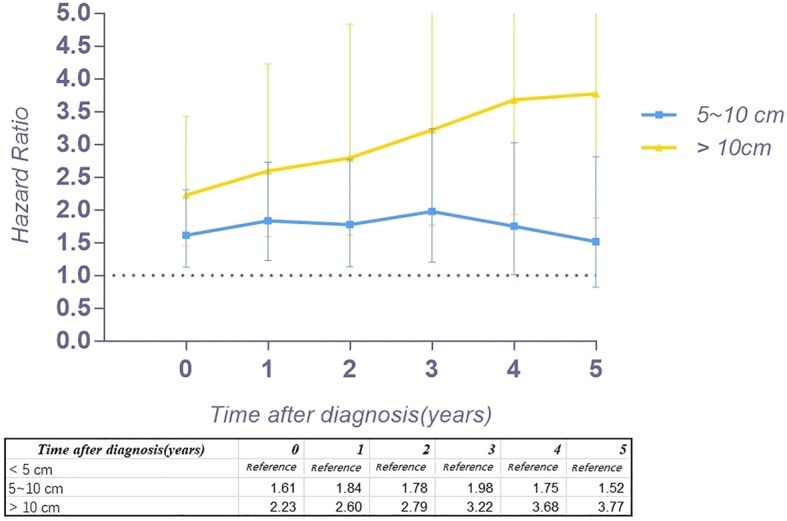
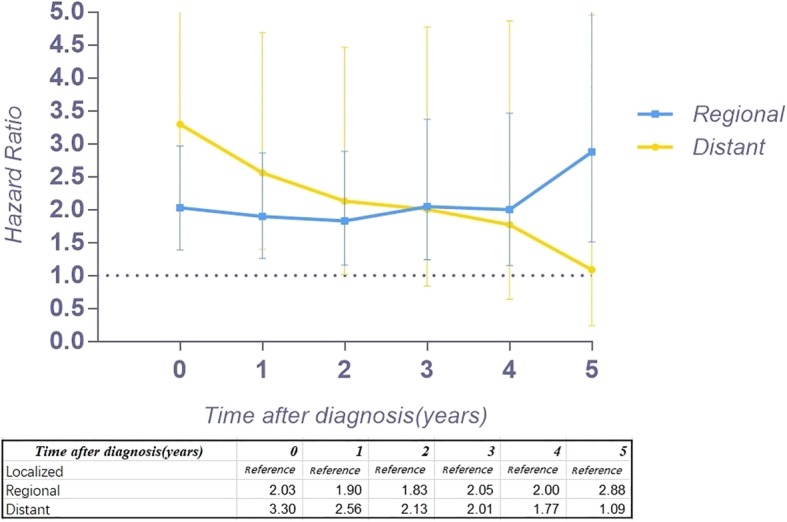
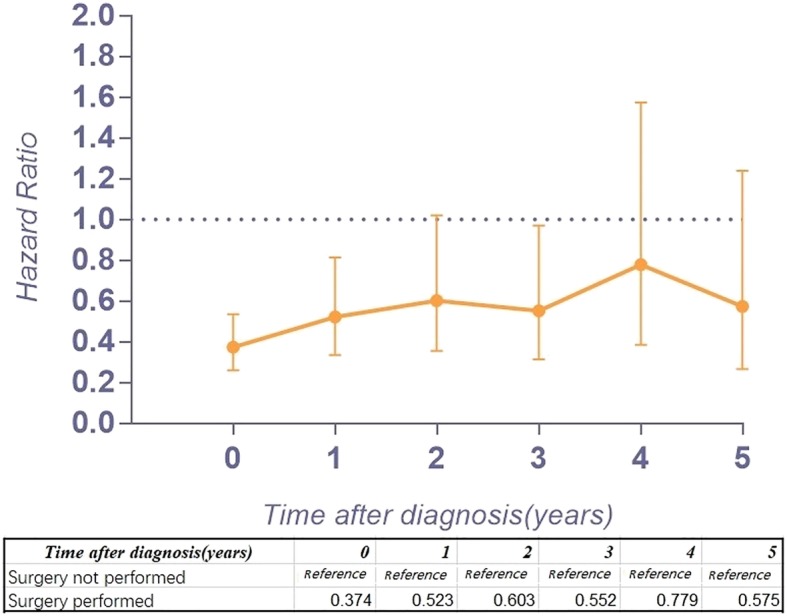
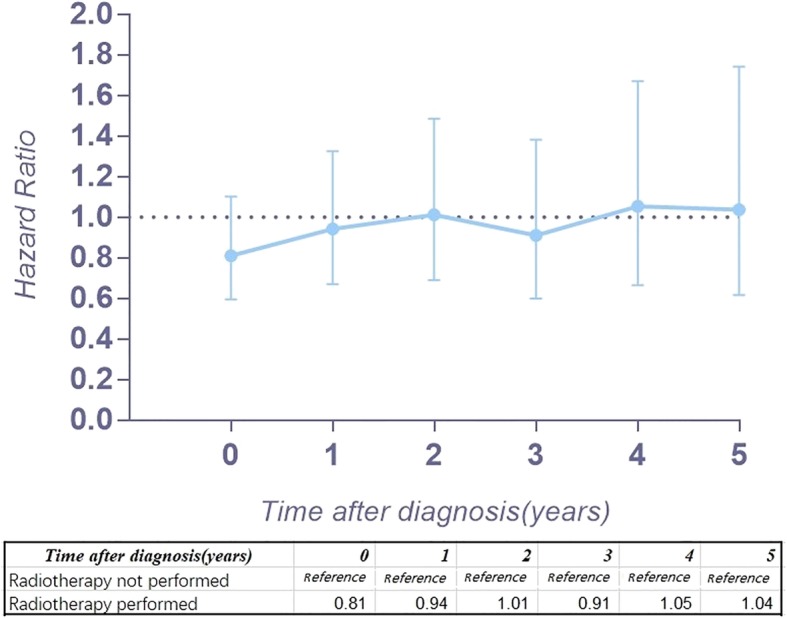
Results: The conditional 5-year disease-specific survival in patients with regional or localized chordoma was relatively stable over time, whereas in patients with distant chordoma, there was a gradual improvement. The conditional 5-year disease-specific survival (DSS) of patients older than 60 years old and patients with a tumor size between 5 and 10 cm improved. Interestingly, for patients with a tumor larger than 10 cm, the conditional 5-year DSS decreased over time. After surviving 5 years, the hazard ratio (HR) of patients older than 60 years old decreased from 1.33 to 1.24, that of patients with a tumor size between 5 and 10 cm decreased from 1.61 to 1.52 and that of patients with distant metastasis decreased from 3.30 to 1.09. However, after surviving 5 years, the HR of patients with a tumor size larger than 10 cm increased from 2.33 to 3.77, that of patients who underwent surgical resection increased from 0.37 to 0.58 and that of patients who received radiation therapy increased from 0.81 to 1.04.
Conclusion: Age at diagnosis, tumor size and disease stage can influence conditional survival for patients with chordoma. The HR of different factors will change over the survival time. Therefore, understanding the changing risk profile and conditional 5-year DSS of chordoma is critical for accurate clinical treatment guidance.
Keywords: Changing risk profile; Chordoma; Conditional survival; Survival.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
MeSH terms
Grants and funding
- RX2016004/Wenzhou leading talent innovative project
- 81501933/National Natural Science Foundation of China
- LY14H060008/Zhejiang Provincial Natural Science Foundation of China
- 2018KY129/Zhejiang Provincial Medical and Health Technology Foundation of China
- Y20170389/Wenzhou Municipal Science and Technology Bureau
LinkOut - more resources
Full Text Sources
Medical
