

Clinical and immunological failure among HIV-positive adults taking first-line antiretroviral therapy in Dire Dawa, eastern Ethiopia
- PMID: 31208459
- PMCID: PMC6580499
- DOI: 10.1186/s12889-019-7078-5
Clinical and immunological failure among HIV-positive adults taking first-line antiretroviral therapy in Dire Dawa, eastern Ethiopia
Abstract
Background: Access to antiretroviral therapy (ART) in Ethiopia has been scaled up since the introduction of the service in 2003. Free ART was launched in 2005, resulting in fewer new human immunodeficiency virus (HIV) infections and deaths from acquired immunodeficiency syndrome (AIDS). However, immunological and clinical failures for first-line ART due to poor adherence and other factors have received less attention. Thus, this study aims to determine the magnitude and associated factors of clinical and immunological failure among HIV-positive adults after six months of first-line ART in Dire Dawa, Eastern Ethiopia.
Methods: A facility-based cross-sectional study was conducted using secondary data of patients on ART in all health facilities providing ART services in Dire Dawa. A total of 949 samples were collected. The data were entered into Epidata version 3.02, and the analysis was performed using SPSS version 16.0. Univariate and multivariate analyses were performed to determine the magnitude of clinical and immunological failure and identify factors significantly associated with the outcome variable.
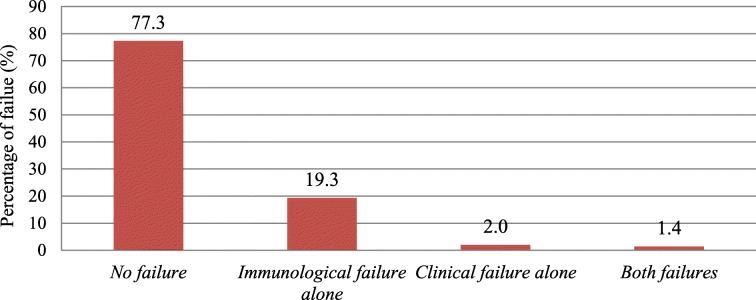
Results: The magnitude of clinical and immunological failure was 22.7% (n = 215). Of these, 33 (15%) patients were switched to second-line ART. CD4 count ≤100 cells/mm3 (AOR: 1.78, 95% CI: 1.18-2.69), poor adherence (AOR: 2.5, 95% CI: 1.19-5.25), restarting after interruption of ART (AOR: 1.93, 95% CI: 1.23-3.07), regimen change (AOR: 1.50, 95% CI: 1.05-2.15), ambulatory/bedridden functional status at the last visit on ART (AOR: 2.41, 95% CI: 1.22-4.75) and patients who died (AOR: 3.94, 95% CI: 1.64-9.45) had higher odds of failure.
Conclusion: The magnitude of clinical and immunological failure was high. To curb this problem, initiation of ART before the occurrence of severe immune suppression, early detection and management of failure and improved adherence support mechanisms are recommended. Restarting treatment after interruption and regimen changes-should-be-made-cautiously.
Keywords: Adherence; Clinical failure; Functional status; Immunological failure.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- UNAIDS. World AIDS day report. Geneva, Switzerland: UNAIDS; 2011. Available from: https://www.unaids.org/sites/default/files/media_asset/JC2216_WorldAIDSd.... Accessed 21 Oct 2018.
-
- World Health Organization, UNAIDS, UNICEF. Global HIV/AIDS response: Epidemic update and health sector progress towards universal access. Progress report. Geneva, Switzerland: WHO; 2011. Available from: https://apps.who.int/iris/bitstream/handle/10665/44787/9789241502986_eng.... Accessed 21 Oct 2018.
-
- FHAPCO. Country progress report on HIV/AIDS response. Addis Ababa, Ethiopia: FHAPCO; 2012. Available from: http://s3.amazonaws.com/zanran_storage/www.unaids.org/ContentPages/25461.... Accessed 21 Oct 2018.
-
- WHO. Antiretroviral therapy for HIV infection in adults and adolescents in resource limited settings: towards universal access. Recommendations for a public health approach. Geneva, Switzerland: WHO; 2006. Available from: https://apps.who.int/iris/bitstream/handle/10665/43554/9789241594677_eng.... Accessed 21 Oct 2018.
-
- FMoH. National Guidelines for Comprehensive HIV Prevention, Care and Treatment in Ethiopia. Addis Ababa, Ethiopia: FMoH; 2014. Available from: https://aidsfree.usaid.gov/sites/default/files/ethiopia_natl_gl_2014.pdf. Accessed 18 Sep 2018.
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
