

Could Treatment Matching Patients' Beliefs About Depression Improve Outcomes?
- PMID: 31208686
- PMCID: PMC6582988
- DOI: 10.1016/j.beth.2018.11.007
Could Treatment Matching Patients' Beliefs About Depression Improve Outcomes?
Abstract
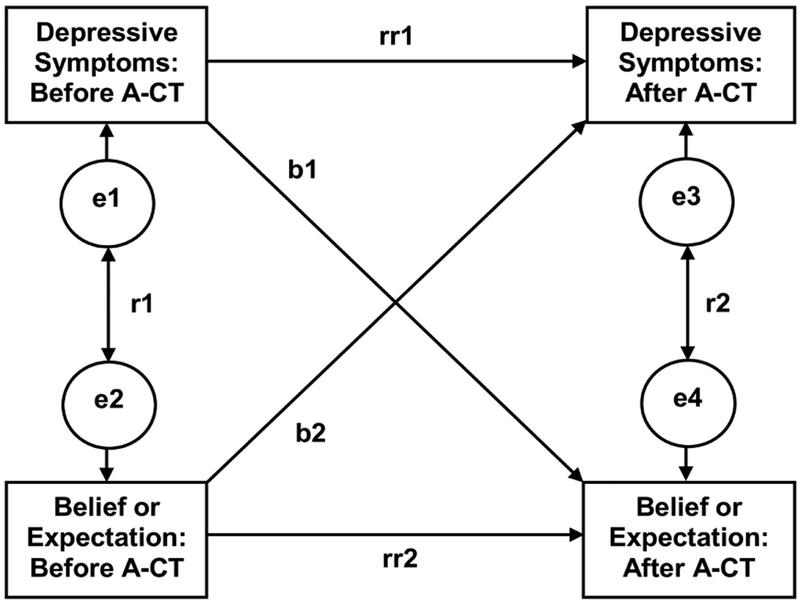
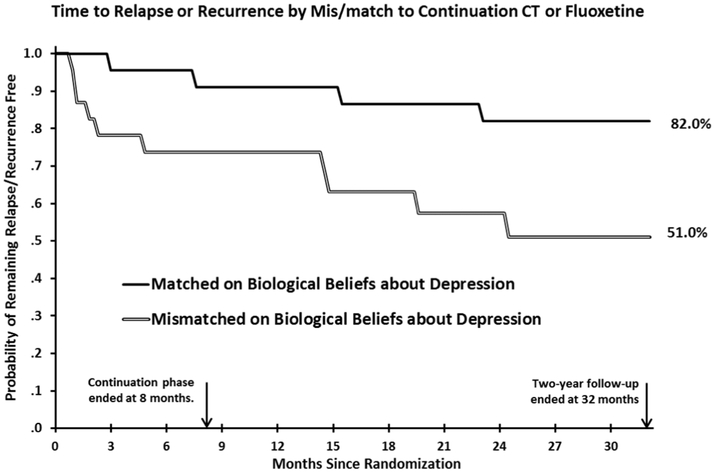
Patients' beliefs about depression and expectations for treatment can influence outcomes of major depressive disorder (MDD) treatments. We hypothesized that patients with weaker biological beliefs (less endorsement of [a] biochemical causes and [b] need for medication) and more optimistic treatment expectations (greater improvement and shorter time to improvement), have better outcomes in cognitive therapy (CT). Outpatients with recurrent MDD who received acute-phase CT (N = 152), and a subset of partial or unstable responders (N = 51) randomized to 8 months of continuation CT or fluoxetine with clinical management, completed repeated measures of beliefs, expectations, and depression. As hypothesized, patients with weaker biological beliefs about depression, and patients who expected a shorter time to improvement, experienced greater change in depressive symptoms and more frequent response to acute-phase CT. Moreover, responders who received continuation treatment better matched to their biological beliefs (i.e., responders with weaker biological beliefs about depression who received continuation CT, or responders with stronger biological beliefs about depression who received continuation fluoxetine) had fewer depressive symptoms and less relapse/recurrence by 32 months after acute-phase CT than did responders who received mismatched continuation treatment. Specific screening and/or intervention targeting patients' biological beliefs about depression could increase CT efficacy.
Keywords: beliefs; cognitive therapy; depression; expectations; relapse.
Copyright © 2019. Published by Elsevier Ltd.
Conflict of interest statement
Declaration of Interests: Dr. Vittengl is a paid reviewer for UpToDate. Dr. Clark has no financial interest or conflict of interest in the research. Dr. Thase has no conflicts of interest pertaining to this paper, although he does report the following relationships with companies that develop treatment for depression or provide education pertaining to those treatments: Dr. Thase has consulted with and/or served on advisory boards for Alkermes, Allergan (includes Forest Laboratories), AstraZeneca, Cerecor, Johnson & Johnson (includes Janssen), Lundbeck, MedAvante, Merck, Moksha8, Otsuka, Pfizer Pharmaceuticals, Shire, Sunovion, and Takeda; he has received grant support from Alkermes, Allergan (includes Forest Laboratories), Assurerx, Johnson & Johnson, Takeda, the Agency for Healthcare Research and Quality, Patient Centered Outcomes Research Institute and the NIMH. He has equity holdings for MedAvante, Inc. and has received royalties from American Psychiatric Publishing, Inc. (APPI), Guilford Publications, Herald House, and W.W. Norton & Company, Inc. Dr. Thase’s spouse is an employee of Peloton Advantage, which does business with several pharmaceutical companies. Dr. Jarrett’s medical center collects the payments from the cognitive therapy she provides to patients. Dr. Jarrett is a paid consultant to the National Institutes of Health and is a paid reviewer for UpToDate.
Figures


References
-
- American Psychiatric Association. (2000). Diagnostic and Statistical Manual of Mental Disorders (4th ed. text rev.). Washington, DC: Author.
-
- Barber JP, Zilcha-Mano S, Gallop R, Barrett M, McCarthy KS, & Dinger U (2014). The associations among improvement and alliance expectations, alliance during treatment, and treatment outcome for major depressive disorder. Psychotherapy Research: Journal of the Society for Psychotherapy Research, 24, 257–268. doi:10.1080/10503307.2013.871080 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
