

Pharmacodynamics of Isavuconazole in a Rabbit Model of Cryptococcal Meningoencephalitis
- PMID: 31209006
- PMCID: PMC6709487
- DOI: 10.1128/AAC.00546-19
Pharmacodynamics of Isavuconazole in a Rabbit Model of Cryptococcal Meningoencephalitis
Abstract
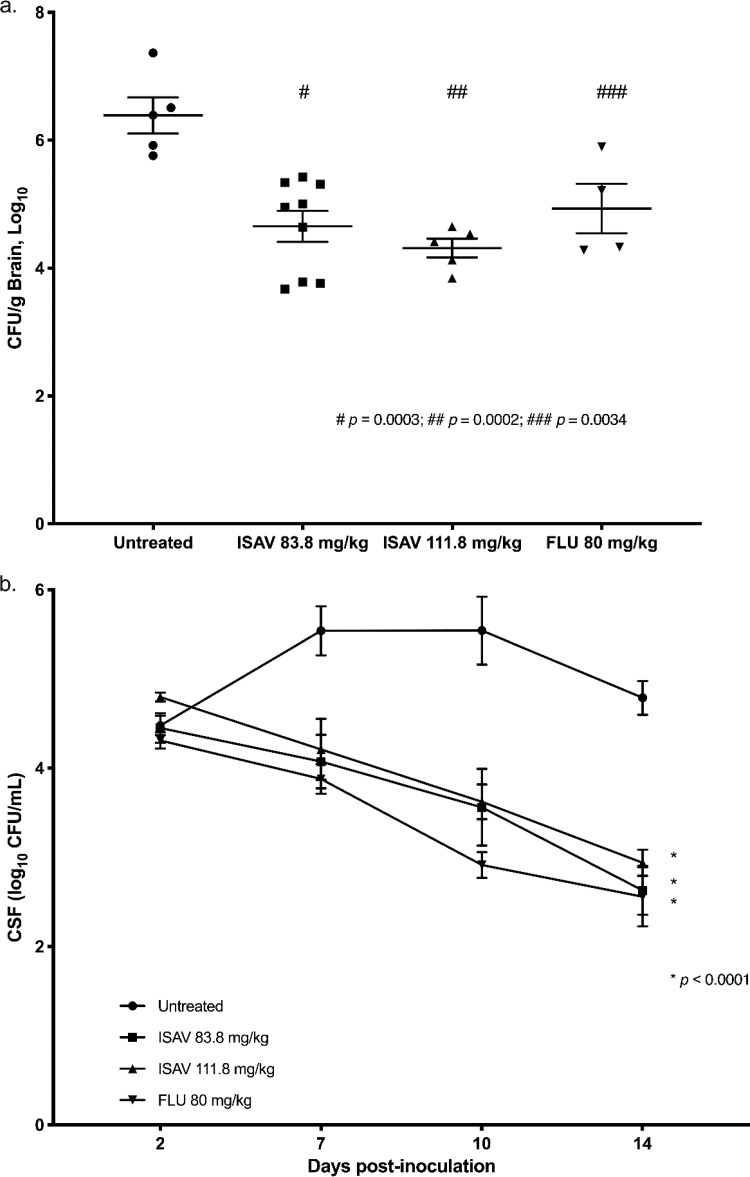
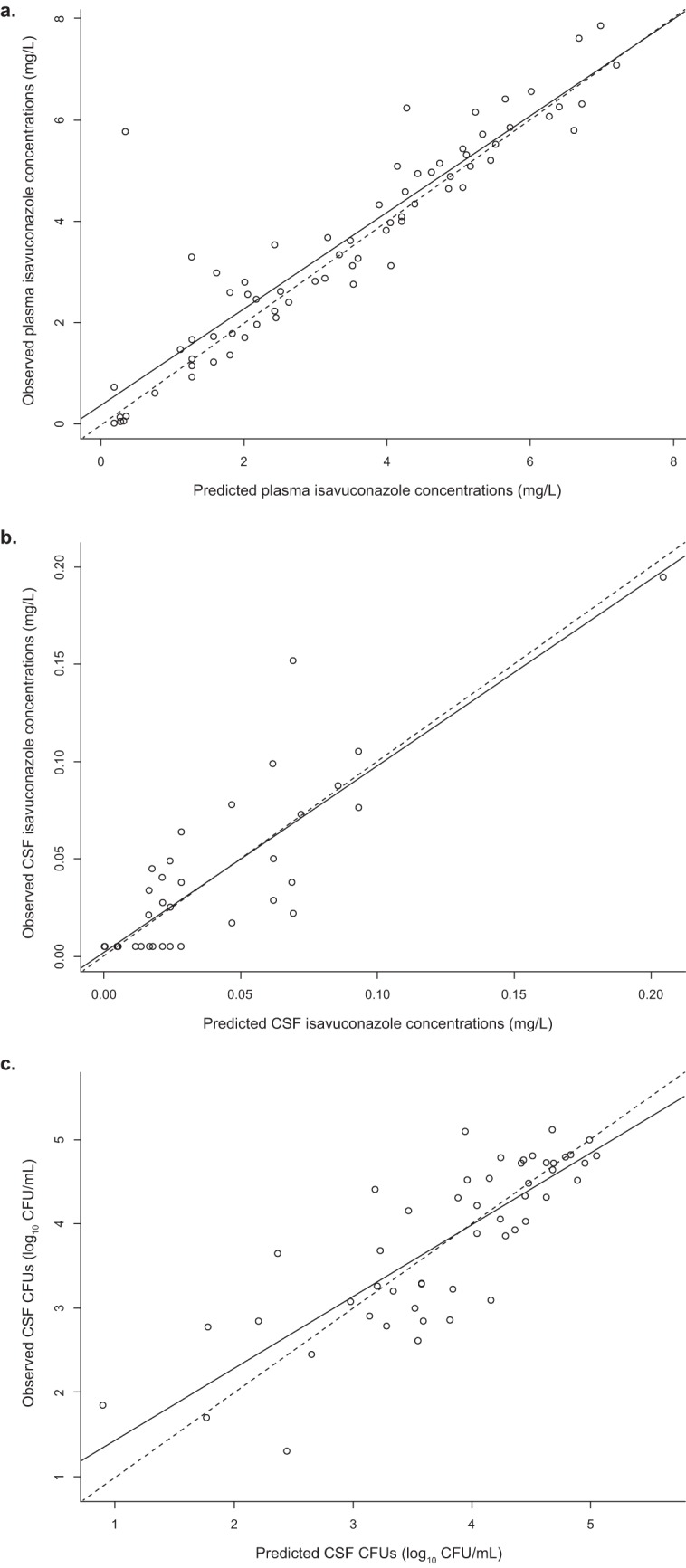
Cryptococcus spp., important fungal pathogens, are the leading cause of fungus-related mortality in human immunodeficiency virus-infected patients, and new therapeutic options are desperately needed. Isavuconazonium sulfate, a newer triazole antifungal agent, was studied to characterize the exposure-response relationship in a rabbit model of cryptococcal meningoencephalitis. Rabbits treated with isavuconazonium sulfate were compared with those treated with fluconazole and untreated controls. The fungal burden in the cerebrospinal fluid was measured serially over time, while the yeast concentrations in the brain and the eye (aqueous humor) were determined at the end of therapy. The exposure impact of isavuconazonium sulfate dosing in the rabbit was linked using mathematical modeling. Similar significant reductions in the fungal burden in the brain and cerebrospinal fluid in rabbits treated with isavuconazonium sulfate and fluconazole compared with that in the untreated controls were observed. No dose-dependent response was demonstrated with isavuconazonium sulfate treatment in this study. The treatment of cryptococcal meningoencephalitis with isavuconazonium sulfate was similar to that with fluconazole. Dose-dependent reductions in yeast over time were not demonstrated, which limited our ability to estimate the pharmacodynamic target. Further nonclinical and clinical studies are needed in order to characterize the extent of the exposure-response relationship in cryptococcal meningoencephalitis. However, this study suggests that isavuconazonium sulfate, like fluconazole, could be beneficial in the setting of consolidation and maintenance therapy, rather than induction monotherapy, in high-burden cryptococcal meningoencephalitis.
Keywords: Cryptococcus neoformans; cryptococcosis; fluconazole; isavuconazole; isavuconazonium sulfate; meningoencephalitis.
Copyright © 2019 Kovanda et al.
Figures
Similar articles
-
Pharmacokinetics and pharmacodynamics of fluconazole for cryptococcal meningoencephalitis: implications for antifungal therapy and in vitro susceptibility breakpoints.Antimicrob Agents Chemother. 2013 Jun;57(6):2793-800. doi: 10.1128/AAC.00216-13. Epub 2013 Apr 9. Antimicrob Agents Chemother. 2013. PMID: 23571544 Free PMC article.
-
Experimental Models of Short Courses of Liposomal Amphotericin B for Induction Therapy for Cryptococcal Meningitis.Antimicrob Agents Chemother. 2017 May 24;61(6):e00090-17. doi: 10.1128/AAC.00090-17. Print 2017 Jun. Antimicrob Agents Chemother. 2017. PMID: 28320715 Free PMC article.
-
Fluconazole Monotherapy Is a Suboptimal Option for Initial Treatment of Cryptococcal Meningitis Because of Emergence of Resistance.mBio. 2019 Dec 3;10(6):e02575-19. doi: 10.1128/mBio.02575-19. mBio. 2019. PMID: 31796539 Free PMC article.
-
Isavuconazonium sulfate: a triazole prodrug for invasive fungal infections.Int J Pharm Pract. 2017 Feb;25(1):18-30. doi: 10.1111/ijpp.12302. Epub 2016 Aug 29. Int J Pharm Pract. 2017. PMID: 27569742 Review.
-
Isavuconazole, a broad-spectrum triazole for the treatment of systemic fungal diseases.Expert Rev Anti Infect Ther. 2015 Jan;13(1):9-27. doi: 10.1586/14787210.2015.990382. Expert Rev Anti Infect Ther. 2015. PMID: 25488140 Review.
Cited by
-
Corticosteroids for Posttransplant Immune Reconstitution Syndrome in Cryptococcus gattii Meningoencephalitis: Case Report and Literature Review.Open Forum Infect Dis. 2019 Oct 23;6(11):ofz460. doi: 10.1093/ofid/ofz460. eCollection 2019 Nov. Open Forum Infect Dis. 2019. PMID: 31737740 Free PMC article.
-
Preclinical Models for Cryptococcosis of the CNS and Their Characterization Using In Vivo Imaging Techniques.J Fungi (Basel). 2024 Feb 12;10(2):146. doi: 10.3390/jof10020146. J Fungi (Basel). 2024. PMID: 38392818 Free PMC article. Review.
-
Isavuconazole-Animal Data and Clinical Data.J Fungi (Basel). 2020 Oct 6;6(4):209. doi: 10.3390/jof6040209. J Fungi (Basel). 2020. PMID: 33036295 Free PMC article. Review.
-
Efficacy of APX2039 in a Rabbit Model of Cryptococcal Meningitis.mBio. 2022 Dec 20;13(6):e0234722. doi: 10.1128/mbio.02347-22. Epub 2022 Oct 12. mBio. 2022. PMID: 36222509 Free PMC article.
-
Efficacy and Associated Drug Exposures of Isavuconazole and Fluconazole in an Experimental Model of Coccidioidomycosis.Antimicrob Agents Chemother. 2021 May 18;65(6):e02344-20. doi: 10.1128/AAC.02344-20. Print 2021 May 18. Antimicrob Agents Chemother. 2021. PMID: 33782009 Free PMC article.
References
-
- World Health Organization. 2018. Guidelines for the diagnosis, prevention and management of cryptococcal disease in HIV-infected adults, adolescents and children: supplement to the 2016 consolidated guidelines on the use of antiretroviral drugs for treating and preventing HIV infection. WHO Guidelines Approved by the Guidelines Review Committee, World Health Organization, Geneva, Switzerland: https://www.ncbi.nlm.nih.gov/books/NBK531449/. Accessed 25 June 2019. - PubMed
-
- Jarvis JN, Bicanic T, Loyse A, Namarika D, Jackson A, Nussbaum JC, Longley N, Muzoora C, Phulusa J, Taseera K, Kanyembe C, Wilson D, Hosseinipour MC, Brouwer AE, Limmathurotsakul D, White N, van der Horst C, Wood R, Meintjes G, Bradley J, Jaffar S, Harrison T. 2014. Determinants of mortality in a combined cohort of 501 patients with HIV-associated cryptococcal meningitis: implications for improving outcomes. Clin Infect Dis 58:736–745. doi:10.1093/cid/cit794. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
