

The combination of complex karyotype subtypes and IGHV mutational status identifies new prognostic and predictive groups in chronic lymphocytic leukaemia
- PMID: 31209327
- PMCID: PMC6738078
- DOI: 10.1038/s41416-019-0502-x
The combination of complex karyotype subtypes and IGHV mutational status identifies new prognostic and predictive groups in chronic lymphocytic leukaemia
Abstract
Background: Complex karyotype (CK) is a heterogeneous category with a negative impact in chronic lymphocytic leukaemia (CLL). Our group has recently reported that CK patients with major structural abnormalities (i.e. CK2) are characterised by a worse prognosis, as compared to other lesions within CK(CK1).
Methods: We performed a multicentre retrospective study to test whether the combination of CK subtypes with IGHV status could be a relevant prognostic and predictive tool.
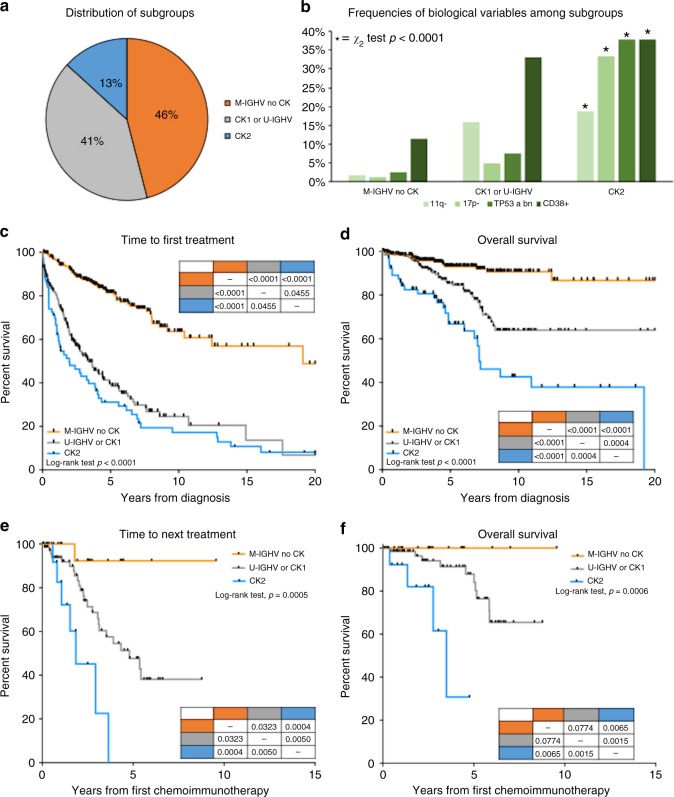
Results: Among 522 patients 13% harboured CK2, 41% CK1 and/or U-IGHV (U-CK1) and 46% M-IGHV without any CK subtypes (M-noCK). After a median follow-up of 5.8 years, CK2 patients had the shortest TTFT (5-year TTFT 31%, 39 and 81%, p < 0.0001) and OS (5-year OS 67%, 85 and 93%, p < 0.0001) as compared to U-CK1 or M-noCK cases, regardless of TP53 abnormalities. CK2 patients also had the worst outcome after chemoimmunotherapy. In fact, the median TTNT after FCR or BR was 1.86 and 4.79 years for CK2 and U-CK1, but not reached for M-noCK patients (p < 0.0005).
Conclusions: We herein suggest that the combined assessment of the IGHV mutational status and CK subtypes refines the prognostication of CLL, allowing to identify M-IGHV patients without any CK subtypes who are characterised by an indolent disease and excellent outcome after chemoimmunotherapy.
Conflict of interest statement
A.V. received honoraria from Janssen and Abbvie. L.T. received research funding by Gilead and Janssen, advisory board for Roche, Shire and Abbvie. G.M.R. received research funding by Gilead. F.R.M. advisory board for Janssen, Shire and Abbvie. A.C. advisory board and speaker bureau for Roche, Abbvie, Gilead and Janssen. G.S. board member of Abbvie, Roche, Janssen and Celgene. R.F. advisory board or speaker bureau for Roche, Abbvie, Celgene, Incyte, Amgen, Janssen, Celtrion, Gilead and Novartis. The remaining authors declare no competing interests.
Figures
References
-
- Visentin A, Facco M, Frezzato F, Castelli M, Trimarco V, Martini V, et al. Integrated CLL scoring system, a new and simple index to predict time to treatment and overall survival in patients with chronic lymphocytic leukemia. Clin. Lymphoma Myeloma Leuk. 2015;15:612–20 e1-5. doi: 10.1016/j.clml.2015.06.001. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
