

Recent advances in invasive adenocarcinoma of the cervix
- PMID: 31209635
- PMCID: PMC6864265
- DOI: 10.1007/s00428-019-02601-0
Recent advances in invasive adenocarcinoma of the cervix
Abstract
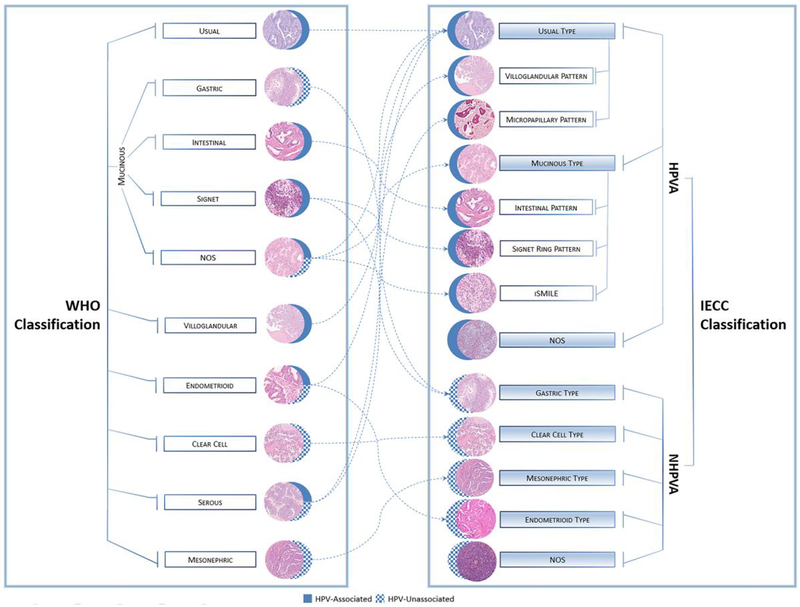
Endocervical adenocarcinomas (ECAs) are currently classified according to the 2014 World Health Organization (WHO) system, which is predominantly based on descriptive morphologic characteristics, considers factors bearing minimal etiological, clinical, or therapeutic relevance, and lacks sufficient reproducibility. The 2017 International Endocervical Adenocarcinoma Criteria and Classification (IECC) system was developed by a group of international collaborators to address these limitations. The IECC system separates ECAs into two major groups-those that are human papillomavirus-associated (HPVA) and those that are non-HPV-associated (NHPVA)-based on morphology (linked to etiology) alone, precluding the need for an expensive panel of immunohistochemical markers for most cases. The major types of HPVA ECA include the usual (with villoglandular and micropapillary architectural variants) and mucinous types (not otherwise specified [NOS], intestinal, signet-ring, and invasive stratified mucin-producing carcinoma). Invasive adenocarcinoma NOS is morphologically uninformative, yet considered part of this group when HPV positive. NHPVA ECAs include gastric, clear cell, endometrioid, and mesonephric types. The IECC system is supported by demographic and clinical features (HPVA ECAs develop in younger patients, are smaller, and are diagnosed at an earlier stage), p16/HPV status (almost all HPVA ECAs are p16 and/or HPV positive), prognostic parameters (NHPVA ECAs more often have lymphovascular invasion, lymph node metastases, and are Silva pattern C), and survival data (NHPVA ECAs are associated with worse survival). A move from the morphology-based WHO system to the IECC system will likely provide clinicians with an improved means to diagnose and classify ECAs, and ultimately, to better personalize treatment for these patients.
Keywords: Classification; Endocervical adenocarcinoma; HPV; International Endocervical Adenocarcinoma Criteria and Classification.
Conflict of interest statement
Figures
References
-
- Kurman RJ, Carcangiu ML, Herrington CS, Young RH (2014) WHO Classification of Tumours of the Female Reproductive Organs, 4th Edition IARC, Lyon
-
- Vesterinen E, Forss M, Nieminen U (1989) Increase of cervical adenocarcinoma: a report of 520 cases of cervical carcinoma including 112 tumors with glandular elements. Gynecol Oncol 33:49–53 - PubMed
