

Analysis of the Clinical Relevance of Histological Classification of Benign Epithelial Salivary Gland Tumours
- PMID: 31209701
- PMCID: PMC6822986
- DOI: 10.1007/s12325-019-01007-3
Analysis of the Clinical Relevance of Histological Classification of Benign Epithelial Salivary Gland Tumours
Abstract
Introduction: A vast increase in knowledge of numerous aspects of malignant salivary gland tumours has emerged during the last decade and, for several reasons, this has not been the case in benign epithelial salivary gland tumours. We have performed a literature review to investigate whether an accurate histological diagnosis of the 11 different types of benign epithelial salivary gland tumours is correlated to any differences in their clinical behaviour.
Methods: A search was performed for histological classifications, recurrence rates and risks for malignant transformation, treatment modalities, and prognosis of these tumours. The search was performed primarily through PubMed, Google Scholar, and all versions of WHO classifications since 1972, as well as numerous textbooks on salivary gland tumours/head and neck/pathology/oncology. A large number of archival salivary tumours were also reviewed histologically.
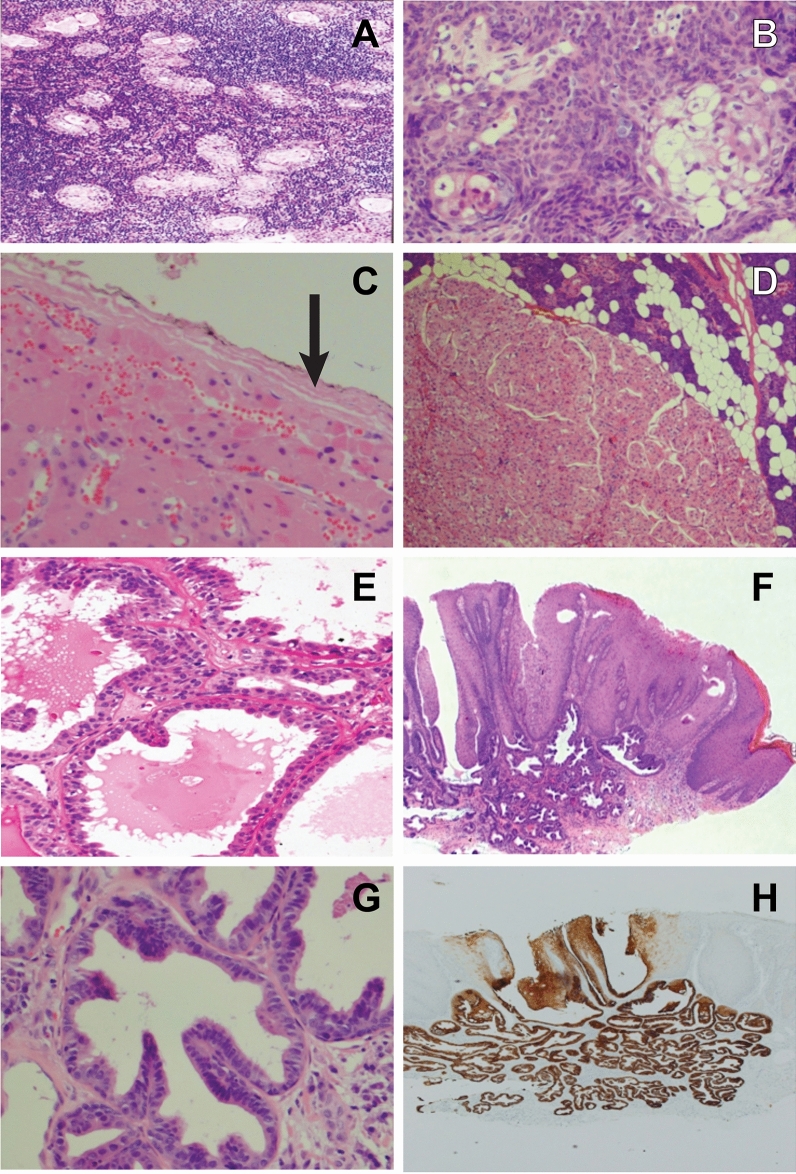
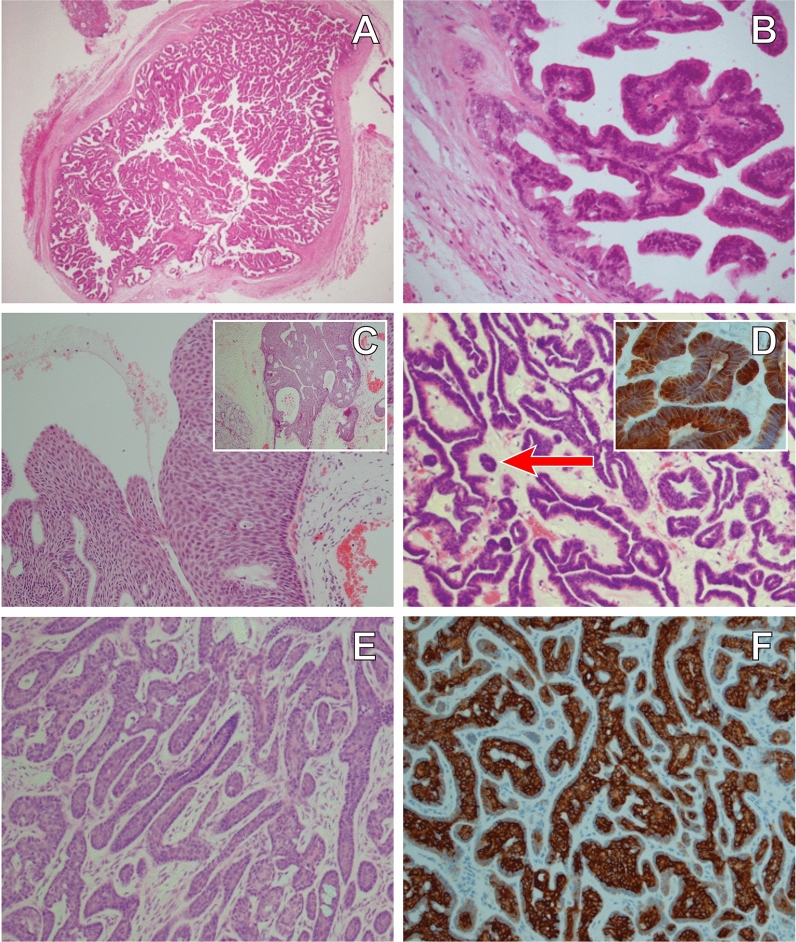
Results: Pleomorphic adenomas carry a considerable risk (5-15%) for malignant transformation but, albeit to a much lesser degree, so do basal cell adenomas and Warthin tumours, while the other eight types virtually never develop into malignancy. Pleomorphic adenoma has a rather high risk for recurrence while recurrence occurs only occasionally in sialadenoma papilliferum, oncocytoma, canalicular adenoma, myoepithelioma and the membranous type of basal cell adenoma. Papillomas, lymphadenoma, sebaceous adenoma, cystadenoma, basal cell adenoma (solid, trabecular and tubular subtypes) very rarely, if ever, recur.
Conclusions: A correct histopathological diagnosis of these tumours is necessary due to (1) preventing confusion with malignant salivary gland tumours; (2) only one (pleomorphic adenoma) has a considerable risk for malignant transformation, but all four histological types of basal cell adenoma can occasionally develop into malignancy, as does Warthin tumour; (3) sialadenoma papilliferum, oncocytoma, canalicular adenoma, myoepithelioma and Warthin tumour only occasionally recur; while (4) intraductal and inverted papilloma, lymphadenoma, sebaceous adenoma, cystadenoma, basal cell adenoma (apart from the membranous type) virtually never recur. No biomarker was found to be relevant for predicting recurrence or potential malignant development. Guidelines for appropriate treatment strategies are given.
Keywords: Benign salivary gland tumours; Biomarkers; Malignant transformation; PubMed; Recurrence; Salivary gland neoplasms; Treatment modalities.
Conflict of interest statement
No named authors (Henrik Hellquist, António Paiva-Correia, Vincent Vander Poorten, Miquel Quer, Juan C. Hernandez-Prera, Simon Andreasen, Peter Zbären, Alena Skalova, Alessandra Rinaldo, or Alfio Ferlito) have any conflicts of interest to declare.
Figures
References
-
- El-Naggar AK, Chan JKC, Grandis JR, Takata T, Slootweg PJ, editors. Tumours of salivary glands. In: WHO classification of head and neck tumours, 4th ed. Lyon: IARC; 2017. p. 159–202.
-
- Thackray AC, Sobin LH, editors. Histological typing of salivary gland tumours. Geneva: WHO; 1972.
-
- Seifert G, Sobin LH, editors. Histological typing of salivary gland tumours. In: WHO international histological classification of tumours. 2nd ed. Berlin: Springer; 1991.
-
- Barnes L, Eveson JW, Reichart P, Sidransky D, editors. Tumours of salivary glands. In: WHO classification of tumours. Pathology and genetics. Head and neck tumours. Lyon: IARC; 2005. p. 209–81.
