

Performance of Controlled Attenuation Parameter in Patients with Advanced Chronic Liver Disease and Portal Hypertension
- PMID: 31209721
- PMCID: PMC6858384
- DOI: 10.1007/s10620-019-05702-7
Performance of Controlled Attenuation Parameter in Patients with Advanced Chronic Liver Disease and Portal Hypertension
Abstract
Background: Liver stiffness (LS) measured by vibration-controlled transient elastography (VCTE) is influenced by liver fibrosis and hepatic perfusion pressure. VCTE-based controlled attenuation parameter (CAP) is a noninvasive marker for hepatic steatosis (HS).
Aims: To investigate the diagnostic performance of CAP in patients with advanced chronic liver disease (ACLD)/portal hypertension (PHT: hepatic venous pressure gradient (HVPG) ≥ 6 mmHg).
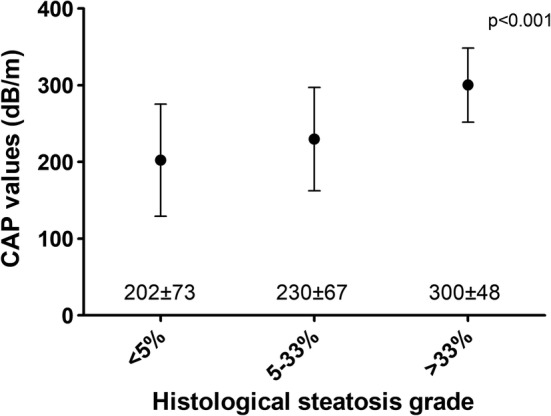
Methods: Eighty-eight patients with LS ≥ 10 kPa and/or HVPG ≥ 6 mmHg who underwent simultaneous liver biopsy, CAP, and HVPG measurement were included. HS was histologically graded according to the modified Brunt classification.
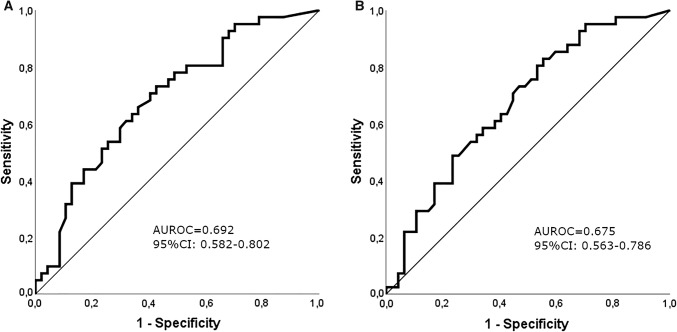
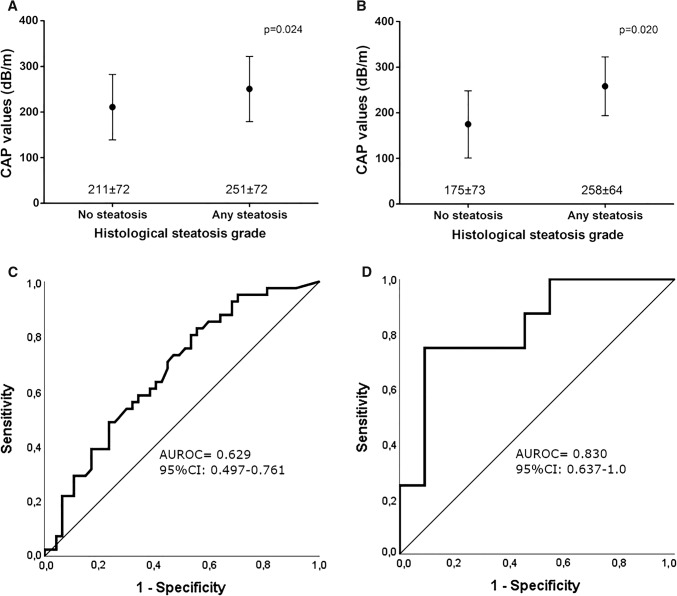
Results: Patient characteristics: Mean MELD:11 (standard derivation [SD] ± 4), median HVPG:16 (interquartile range [IQR]10-19) mmHg, median LS:27.4 (IQR 16.2-48.9) kPa, and mean CAP:221 (SD ± 75) dB/m. According to histology, 47 (53.4%) patients had no HS (S0), 28 (31.8%) had S1, 11 (12.5%) had S2, and 2 (2.3%) had S3. The area under the receiver operating characteristic curve (AUROC) of CAP for diagnosing any HS (S0 vs. ≥ S1) was 0.692 (95% confidence interval [95% CI] 0.582-0.802) in the overall cohort, 0.830 (95% CI 0.637-1.0) in patients with HVPG < 10 mmHg, and 0.629 (95% CI 0.497-0.761) in patients with clinically significant portal hypertension (CSPH; HVPG ≥ 10 mmHg; n = 69). Using the established cutoff for any HS (248 dB/m), the sensitivity/specificity of CAP was only 48.8%/76.6%, respectively. In contrast, the AUROC and sensitivity/specificity (cutoff 268 dB/m) for diagnosing HS ≥ S2 were 0.842 (95% CI 0.747-0.936) and 84.6%/81.3%, respectively. CAP correlated with the percentage of steatotic hepatocytes (Spearman's ρ = 0.402; p ≤ 0.001) and showed a weak correlation with liver stiffness (ρ = 0.225; p = 0.035).
Conclusions: The diagnostic performance of CAP for any HS seems to be limited in patients with ACLD, if CSPH is present.
Keywords: CAP; CSPH; Cirrhosis; Portal hypertension; Transient elastography; VCTE.
Conflict of interest statement
The authors have nothing to disclose regarding the work under consideration for publication. The following authors disclose conflicts of interests outside the submitted work: JS received grant support from Gilead, Eli, and Lilly. BS received travel support from Gilead. PS received speaker fees from Boehringer Ingelheim and travel support from Boehringer Ingelheim and Gilead. MP received speaker fees from Bayer and Bristol-Myers Squibb, travel support from Bayer, and served as advisory board member for Bayer, Bristol-Myers Squibb, and Eisai. AF has served as a speaker and consultant for AbbVie, Gilead, and Intercept and owns a patent on a catheter for the measurement of hepatic venous pressure gradient. MT received speaker fees from Gilead and MSD, travel support from Gilead, grant support from MSD, and honoraria for consulting from AbbVie, Gilead, Janssen, and MSD. TR received speaker fees from Boehringer Ingelheim, Gore, and MSD, travel support from Boehringer Ingelheim, Gilead, MSD, and Gore, grant support from AbbVie, Boehringer Ingelheim, Boston Scientific, Cook Medical, Gilead, Gore, Guerbet, Phenex Pharmaceuticals, Philips, and MSD, and served as a consultant for AbbVie, Bayer, Boehringer Ingelheim, Gilead, and MSD. MM served as a speaker and consultant for AbbVie, Bristol-Myers Squibb, Gilead, Gore, and Janssen. GS, RP, KW, and AFS have nothing to disclose.
Figures
References
-
- de Franchis R. Expanding consensus in portal hypertension: report of the Baveno VI consensus workshop: stratifying risk and individualizing care for portal hypertension. J Hepatol. 2015;63:743–752. - PubMed
-
- Mandorfer M, Bota S, Schwabl P, et al. Nonselective beta blockers increase risk for hepatorenal syndrome and death in patients with cirrhosis and spontaneous bacterial peritonitis. Gastroenterology. 2014;146:1681–1690. - PubMed
-
- Younossi ZM, Koenig AB, Abdelatif D, Fazel Y, Henry L, Wymer M. Global epidemiology of nonalcoholic fatty liver disease-meta-analytic assessment of prevalence, incidence, and outcomes. Hepatology (Baltimore, Md.) 2016;64:73–84. - PubMed
-
- Bedossa P, Carrat F. Liver biopsy: the best, not the gold standard. J Hepatol. 2009;50:1–3. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
