Delay in diagnosis of thoracolumbar fractures
- PMID: 31210909
- PMCID: PMC6551460
- DOI: 10.4081/or.2019.7774
Delay in diagnosis of thoracolumbar fractures
Abstract
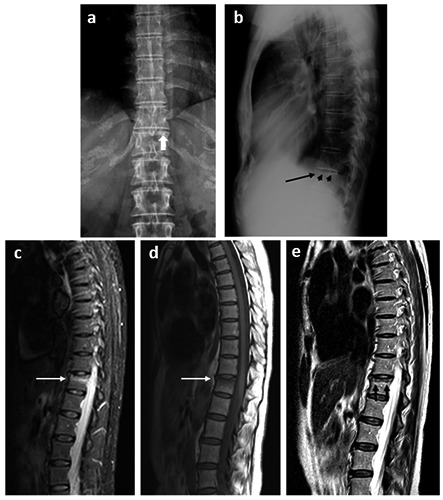
The time interval between the date of trauma and the diagnosis of vertebral column fractures hinders management and increases liability. We have examined the features and implications of this delay. 585 consecutive thoracolumbar fractures (2005-2016), were considered; 382 (65.30%) were males and 203 (34.70%) females. Mean age was 51 yr. Fall from a height (187; 31.97%), simple fall (147; 25.13%) and road accidents (111; 18.97%) were the most frequent causes of trauma. Physical exertion caused 8.38% (N=49). 142 patients (24.27%) were not diagnosed on the injury day (mean = 3.2 days). Delay was longer in females (mean = 5.5 vs. 2.7 days) and shorter in falls from a height (mean = 2.3) or road accidents (2.8). Mean age of diagnosed on the injury day differed from those diagnosed in the first month (49.2 vs 60.1). Plain X-ray signs were found in 7 misdiagnosed cases (46.6%). Delay was more frequent in low mineralization cases. Diagnostic delay of spine fractures is frequent. Some risk profiles can help to reduce it. Careful emergency X-ray examination is encouraged, as well as early magnetic resonance imaging in risk profiles.
Keywords: Diagnostic delay; Misdiagnosis; Osteoporosis; Vertebral fractures.
Conflict of interest statement
Conflict of interest: the authors declare no potential conflict of interest.
Figures
References
-
- Karlsson MK, Kherad M, Hasserius R, et al. Characteristics of prevalent vertebral fractures predict new fractures in elderly men. J Bone Joint Surg Am 2016;98:379-85. - PubMed
-
- Pongchaiyakul C, Nguyen ND, Jones G, et al. Asymptomatic vertebral deformity as a major risk factor for subsequent fractures and mortality: a longterm prospective study. J Bone Miner Res 2005;20:1349-55. - PubMed
-
- Bernstein M. Easily missed thoracolumbar spine fractures. Eur J Radiol 2010;74:6-15. - PubMed
LinkOut - more resources
Full Text Sources