

Adverse Outcomes Associated With Potentially Inappropriate Antibiotic Use in Heart Failure Admissions
- PMID: 31211161
- PMCID: PMC6559271
- DOI: 10.1093/ofid/ofz220
Adverse Outcomes Associated With Potentially Inappropriate Antibiotic Use in Heart Failure Admissions
Abstract
Background: Acute decompensated heart failure (ADHF) can be confused with other conditions that cause dyspnea. Patients with ADHF are often simultaneously treated for community-acquired pneumonia (CAP), even when evidence for infection is lacking. We hypothesized that the fluid and sodium content of potentially unnecessary intravenous antibiotic (IVAB) therapy could worsen outcomes of ADHF patients.
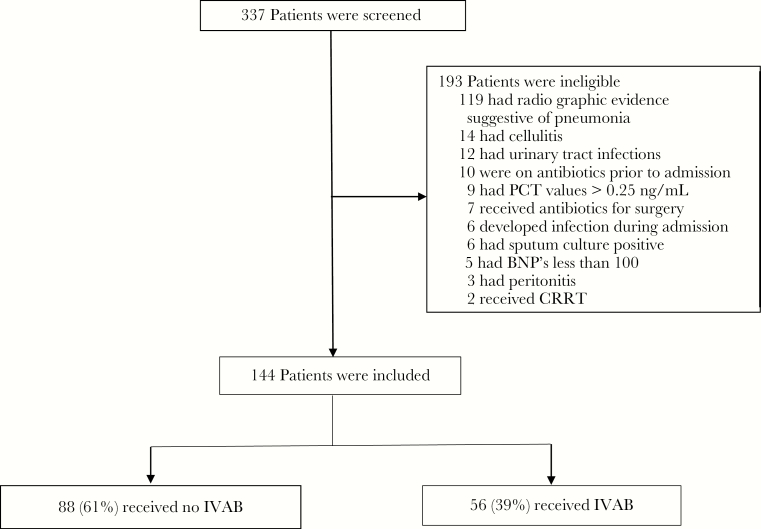
Methods: We reviewed 144 ADHF patients at low risk of pneumonia based on diagnostic findings and clinical documentation. The primary end point was length of stay. Secondary outcomes were mortality, readmission rates, amount of diuretic received, and fluid volume and quantity of sodium administered as part of IVAB therapy.
Results: Of the 144 admissions reviewed, 88 did not and 56 did receive IVAB. IVAB-treated patients received an average of 1.7 L of additional fluid (230 mL/d) and 9311 mg of additional sodium (1381 mg/d) as a result of IVAB therapy. Length of stay was longer in the IVAB arm (6.6 days) compared with the no-IVAB arm (3.0 days; P < .001). Patients required more furosemide in the IVAB arm (930 mg) compared with the no-IVAB arm (320 mg; P < .001). Patients who received IVAB were also 2.51 times more likely to be readmitted compared with patients who did not receive IVAB (P = .04).
Conclusions: ADHF patients who received IVAB without evidence of infection had longer lengths of stay, required more diuretics, and were more likely to be readmitted compared with ADHF patients not exposed to IVAB. ADHF patients are a promising target of antibiotic stewardship interventions.
Keywords: antibiotic stewardship; heart failure; pneumonia; procalcitonin; sodium.
Figures
References
-
- McMurray JJ, Petrie MC, Murdoch DR, Davie AP. Clinical epidemiology of heart failure: public and private health burden. Eur Heart J 1998; 19(Suppl P):P9–16. - PubMed
-
- Owan TE, Redfield MM. Epidemiology of diastolic heart failure. Prog Cardiovasc Dis 2005; 47:320–32. - PubMed
-
- Christ-Crain M, Stolz D, Bingisser R, et al. . Procalcitonin guidance of antibiotic therapy in community-acquired pneumonia: a randomized trial. Am J Respir Crit Care Med 2006; 174:84–93. - PubMed
-
- Schuetz P, Christ-Crain M, Thomann R, et al. ; ProHOSP Study Group Effect of procalcitonin-based guidelines vs standard guidelines on antibiotic use in lower respiratory tract infections: the ProHOSP randomized controlled trial. JAMA 2009; 302:1059–66. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
