

Phenotype-genotype discrepancies in the prospective Huntington at-risk observational study
- PMID: 31211168
- PMCID: PMC6562068
- DOI: 10.1002/acn3.781
Phenotype-genotype discrepancies in the prospective Huntington at-risk observational study
Abstract
Objective: To examine phenotype-genotype discrepancies (PGDs) wherein genotype-concealed and prospective judgments of the motor onset of Huntington disease (HD) occurred among at-risk adults who had nonexpanded (<37) cytosine-adenine-guanine (CAG) trinucleotide DNA repeats.
Methods: We examined the prospective clinical assessments of investigators who were kept unaware of individual CAG lengths in the Prospective Huntington At-Risk Observational Study (PHAROS) who enrolled and followed undiagnosed adults at risk for HD who chose not to learn their gene status. Subjects (n = 1001) at 43 Huntington Study Group research sites in the US and Canada were evaluated prospectively and systematically between 1999 and 2009. At each site, an investigator was designated to perform comprehensive clinic assessments and another investigator to rate only the motor examination. Phenoconversion from a "premanifest" status to a confidently "manifest" status was based on investigator judgment (diagnostic confidence level) of the extrapyramidal motor features of HD.
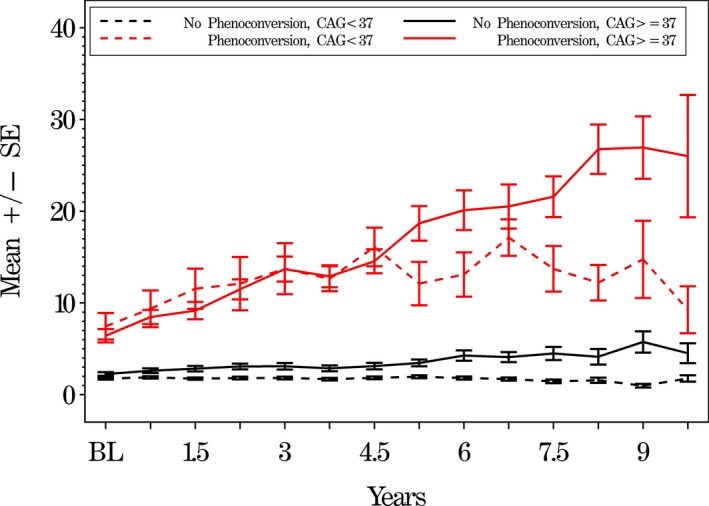
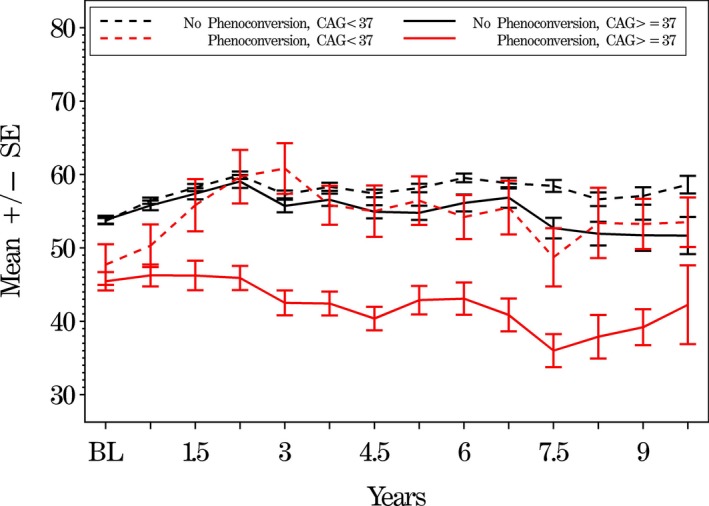
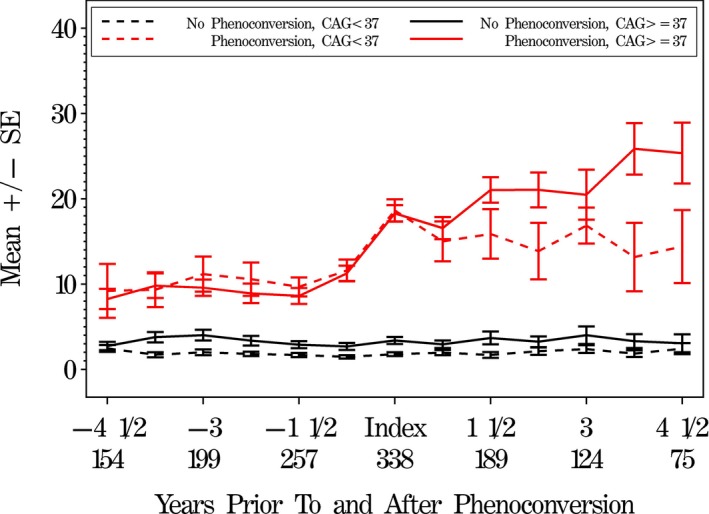
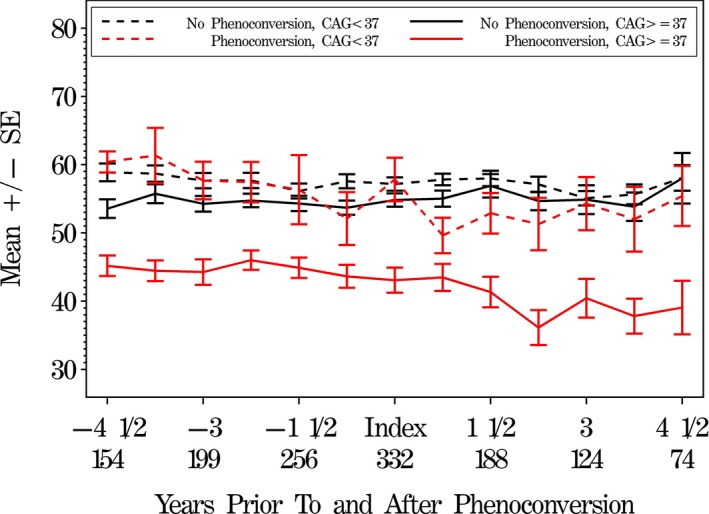
Results: There were 20 PGDs that over time had less severe motor scores than the 101 phenoconversions with CAG ≥37, but more severe motor scores than nonconversions. Following conversion, subjects with CAG ≥37 expansions worsened more motorically and cognitively than PGD subjects in the < 37 group. PGDs were concentrated among three sites and a few investigators, especially raters who only assessed the motor examination.
Interpretation: The ability to detect the clinical onset of HD in a timely and reliable fashion remains the key for developing experimental treatments aimed at postponing the clinical onset of HD. Comprehensive clinical evaluation is a more accurate and reliable basis for determining HD clinical onset than sole reliance on judging the extrapyramidal features of HD.
Conflict of interest statement
None of the authors report conflicts of interest related to the conduct or reporting of PHAROS.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
