

A Pilot Study on Histopathology of the Jejunoileal Atresia-Can it Be Used as a Guide to Determine the Length of Adequate Resection?
- PMID: 31211290
- PMCID: PMC6546944
- DOI: 10.1177/2632010X19829263
A Pilot Study on Histopathology of the Jejunoileal Atresia-Can it Be Used as a Guide to Determine the Length of Adequate Resection?
Abstract
Introduction: Some studies reported that there is abnormality in the histopathology of atretic bowel in jejunoileal atresia (JIA). We have made an attempt to assess sequential histopathologic changes in the resected atretic segment.
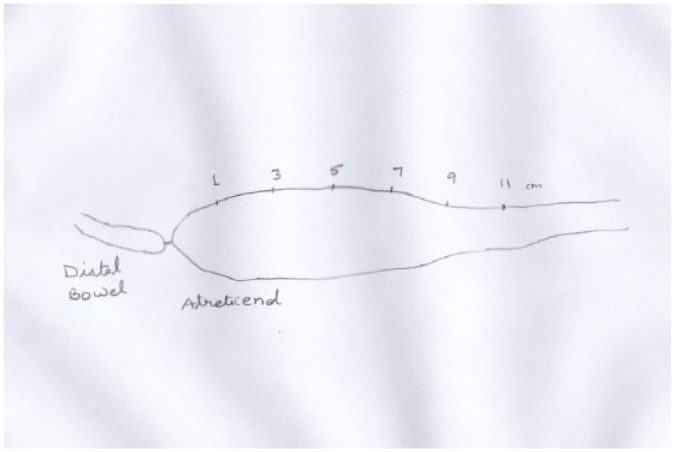
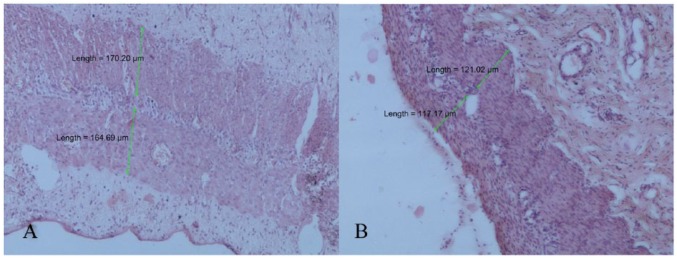
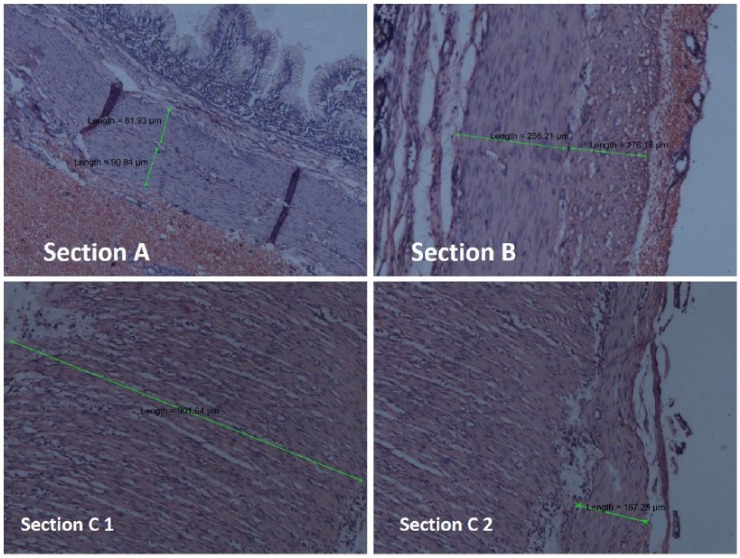
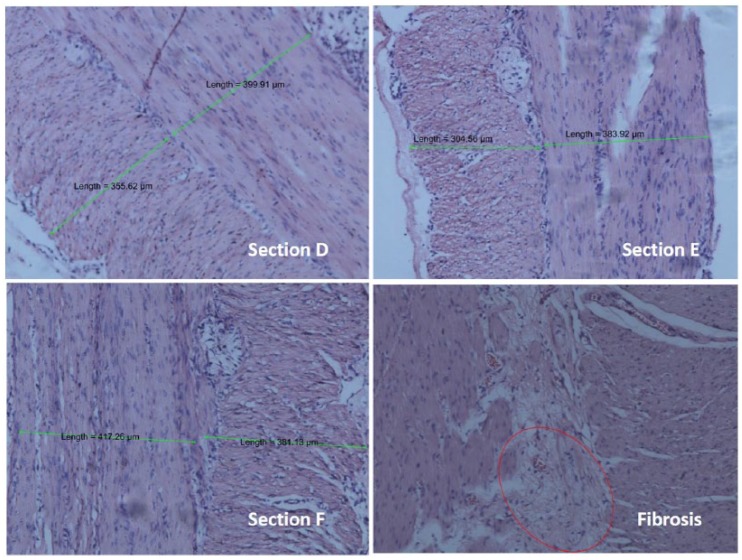
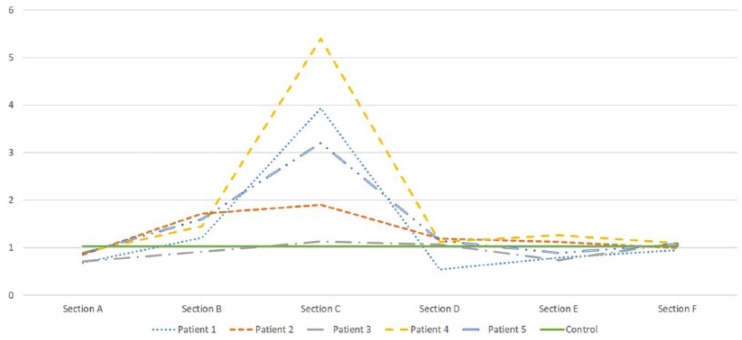
Material and methods: The histopathology of the resected segment was evaluated at 1, 3, 5, 7, 9, and 11 cm from atretic end (Sections A to F, respectively). The ratio of inner and outer muscle layer (measured by NIS-Element D software) was calculated at every section. Immunohistochemistry for α-smooth muscle actin (α-SMA) was also done. The findings were compared with control.
Results: In control set (n = 5), the ratio of inner and outer muscle layer was 1.03. In patients with JIA, the ratio was 0.68 to 0.9 at section A. This ratio varied at various sections in all specimens. In section F, this ratio was 0.95 to 1.09, which is close to control ratio. There were no specific findings related to α-SMA staining.
Conclusions: It appears that the bowel proximal to the atresia is abnormal for a varied length. It may be a possibility that this abnormality is present at least up to about 10 cm proximal to atresia. Adequate resection is important for optimal outcome.
Keywords: Atresia; histopathology; jejunoileal atresia.
Conflict of interest statement
Declaration of conflicting interests:The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures
Similar articles
-
Novel insights into the histology of jejunoileal atresia and its therapeutic implications.J Pediatr Surg. 2020 Dec;55(12):2630-2634. doi: 10.1016/j.jpedsurg.2020.05.006. Epub 2020 May 11. J Pediatr Surg. 2020. PMID: 32534904
-
Clinicopathological study of intestinal smooth muscles, interstitial cells of Cajal, and enteric neurons in neonatal jejuno-ileal atresia with special reference to muscle morphometry.J Pediatr Surg. 2019 Nov;54(11):2291-2299. doi: 10.1016/j.jpedsurg.2019.06.003. Epub 2019 Jun 19. J Pediatr Surg. 2019. PMID: 31257016
-
Morphological abnormalities in the innervation of the atretic segment of bowel in neonates with intestinal atresia.Pediatr Surg Int. 2007 Dec;23(12):1183-6. doi: 10.1007/s00383-007-2029-0. Pediatr Surg Int. 2007. PMID: 17955249
-
Intestinal atresia and stenosis: a 25-year experience with 277 cases.Arch Surg. 1998 May;133(5):490-6; discussion 496-7. doi: 10.1001/archsurg.133.5.490. Arch Surg. 1998. PMID: 9605910 Review.
-
Follicular atresia in pigs: measurement and physiology.J Anim Sci. 1995 Sep;73(9):2834-44. doi: 10.2527/1995.7392834x. J Anim Sci. 1995. PMID: 8582874 Review.
References
-
- Frischer JS, AzizKhan RG. Jejunoileal atresia and stenosis. In: Coran AG, Krummel TM, Laberge J, Shamberger RC, Caldamone AA, eds. Pediatric Surgery. 7th ed. Philadelphia, PA: W.B. Saunders; 2012:1059-1071.
-
- Masumoto K, Suita S, Nada O, Taguchi T, Guo R. Abnormalities of enteric neurons, intestinal pacemaker cells, and smooth muscle in human intestinal atresia. J Pediatr Surg. 1999;34:1463-1468. - PubMed
-
- Ozguner IF, Savas C, Ozguner M, Candir O. Intestinal atresia with segmental musculature and neural defect. J Pediatr Surg. 2005;40:1232-1237. - PubMed
-
- Ramachandran P, Vincent P, Ganesh S, Sridharan S. Morphological abnormalities in the innervation of the atretic segment of bowel in neonates with intestinal atresia. Pediatr Surg Int. 2007;23:1183-1186. - PubMed
-
- Tander B, Bicakci U, Sullu Y, et al. Alterations of Cajal cells in patients with small bowel atresia. J Pediatr Surg. 2010;45:724-728. - PubMed
LinkOut - more resources
Full Text Sources
