

Preformed Donor-Specific HLA Antibodies in Living and Deceased Donor Transplantation: A Multicenter Study
- PMID: 31213508
- PMCID: PMC6625630
- DOI: 10.2215/CJN.13401118
Preformed Donor-Specific HLA Antibodies in Living and Deceased Donor Transplantation: A Multicenter Study
Abstract
Background and objectives: The prognostic value of preformed donor-specific HLA antibodies (DSA), which are only detectable by sensitive methods, remains controversial for kidney transplantation.
Design, setting, participants, & measurements: The outcome of 4233 consecutive kidney transplants performed between 2012 and 2015 in 18 German transplant centers was evaluated. Most centers used a stepwise pretransplant antibody screening with bead array tests and differentiation of positive samples by single antigen assays. Using these screening results, DSA against HLA-A, -B, -C, -DRB1 and -DQB1 were determined. Data on clinical outcome and possible covariates were collected retrospectively.
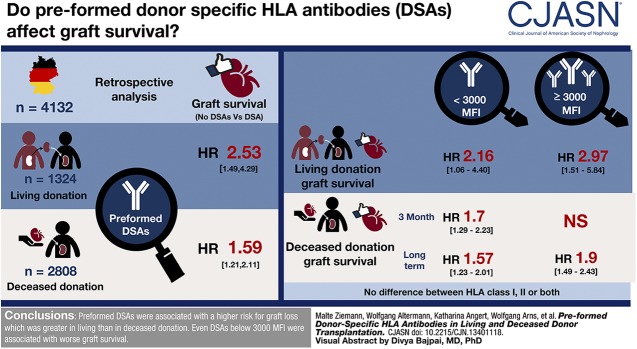
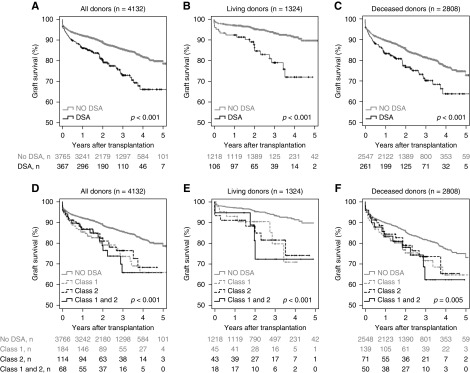
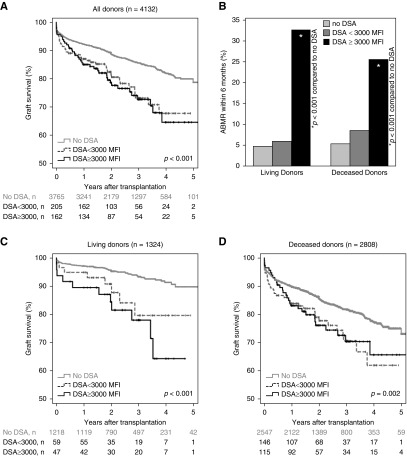
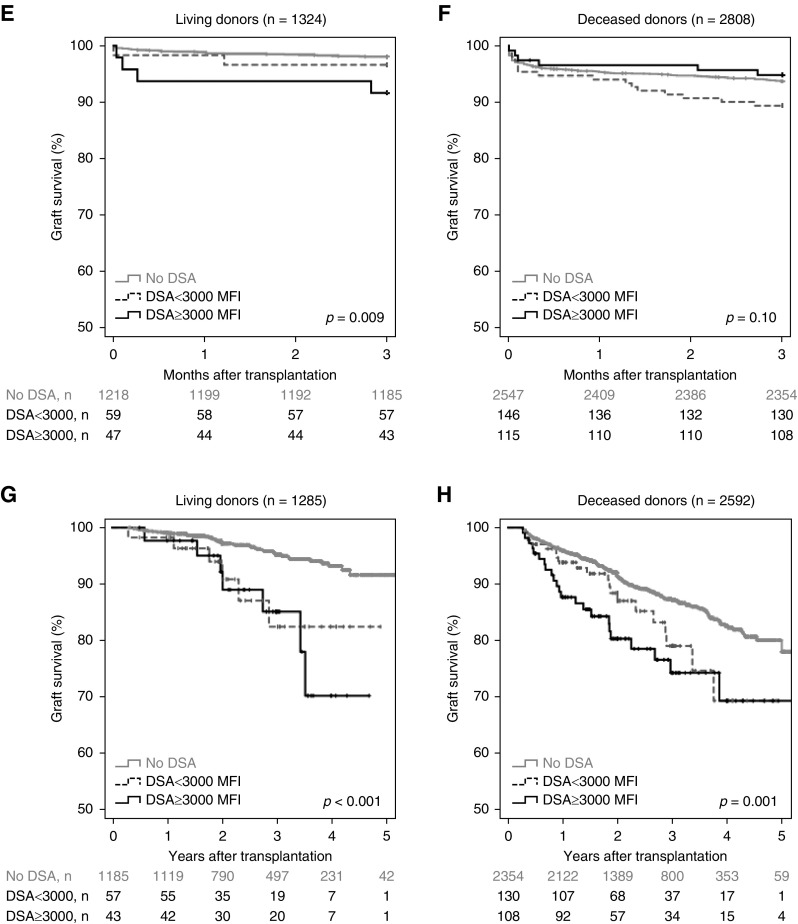
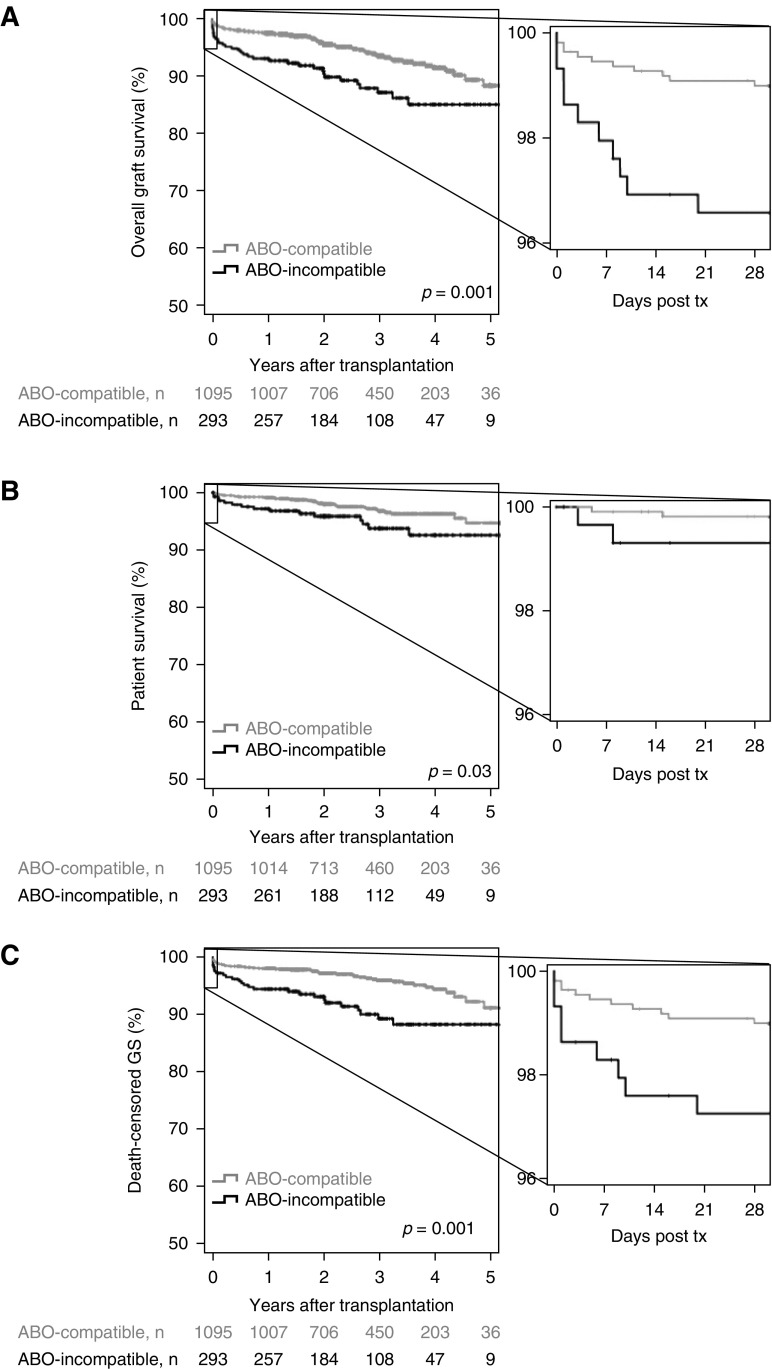
Results: Pretransplant DSA were associated with lower overall graft survival, with a hazard ratio of 2.53 for living donation (95% confidence interval [95% CI], 1.49 to 4.29; P<0.001) and 1.59 for deceased donation (95% CI, 1.21 to 2.11; P=0.001). ABO-incompatible transplantation was associated with worse graft survival (hazard ratio, 2.09; 95% CI, 1.33 to 3.27; P=0.001) independent from DSA. There was no difference between DSA against class 1, class 2, or both. Stratification into DSA <3000 medium fluorescence intensity (MFI) and DSA ≥3000 MFI resulted in overlapping survival curves. Therefore, separate analyses were performed for 3-month and long-term graft survival. Although DSA <3000 MFI tended to be associated with both lower 3-month and long-term transplant survival in deceased donation, DSA ≥3000 MFI were only associated with worse long-term transplant survival in deceased donation. In living donation, only strong DSA were associated with reduced graft survival in the first 3 months, but both weak and strong DSA were associated with reduced long-term graft survival. A higher incidence of antibody-mediated rejection within 6 months was only associated with DSA ≥3000 MFI.
Conclusions: Preformed DSA were associated with an increased risk for graft loss in kidney transplantation, which was greater in living than in deceased donation. Even weak DSA <3000 MFI were associated with worse graft survival. This association was stronger in living than deceased donation.
Keywords: ABO-incompatible transplantation; Antibodies; Fluorescence; HLA-A Antigens; Incidence; Prognosis; Retrospective Studies; Tissue Donors; donor-specific HLA antibodies; graft survival; kidney transplantation; preformed HLA antibodies.
Copyright © 2019 by the American Society of Nephrology.
Figures
Comment in
-
Clinical and Public Policy Implications of Pre-Formed DSA and Transplant Outcomes.Clin J Am Soc Nephrol. 2019 Jul 5;14(7):972-974. doi: 10.2215/CJN.05950519. Epub 2019 Jun 18. Clin J Am Soc Nephrol. 2019. PMID: 31213509 Free PMC article. No abstract available.
References
-
- Patel R, Terasaki PI: Significance of the positive crossmatch test in kidney transplantation. N Engl J Med 280: 735–739, 1969 - PubMed
-
- Tait BD, Süsal C, Gebel HM, Nickerson PW, Zachary AA, Claas FHJ, Reed EF, Bray RA, Campbell P, Chapman JR, Coates PT, Colvin RB, Cozzi E, Doxiadis II, Fuggle SV, Gill J, Glotz D, Lachmann N, Mohanakumar T, Suciu-Foca N, Sumitran-Holgersson S, Tanabe K, Taylor CJ, Tyan DB, Webster A, Zeevi A, Opelz G: Consensus guidelines on the testing and clinical management issues associated with HLA and non-HLA antibodies in transplantation. Transplantation 95: 19–47, 2013 - PubMed
-
- Loupy A, Lefaucheur C, Vernerey D, Prugger C, Duong van Huyen J-P, Mooney N, Suberbielle C, Frémeaux-Bacchi V, Méjean A, Desgrandchamps F, Anglicheau D, Nochy D, Charron D, Empana JP, Delahousse M, Legendre C, Glotz D, Hill GS, Zeevi A, Jouven X: Complement-binding anti-HLA antibodies and kidney-allograft survival. N Engl J Med 369: 1215–1226, 2013 - PubMed
-
- Schinstock CA, Gandhi M, Cheungpasitporn W, Mitema D, Prieto M, Dean P, Cornell L, Cosio F, Stegall M: Kidney transplant with low levels of DSA or low positive B-flow crossmatch: An underappreciated option for highly sensitized transplant candidates. Transplantation 101: 2429–2439, 2017 - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
