

Cervical Cancer, Different Treatments and Importance of Bile Acids as Therapeutic Agents in This Disease
- PMID: 31214018
- PMCID: PMC6558109
- DOI: 10.3389/fphar.2019.00484
Cervical Cancer, Different Treatments and Importance of Bile Acids as Therapeutic Agents in This Disease
Abstract
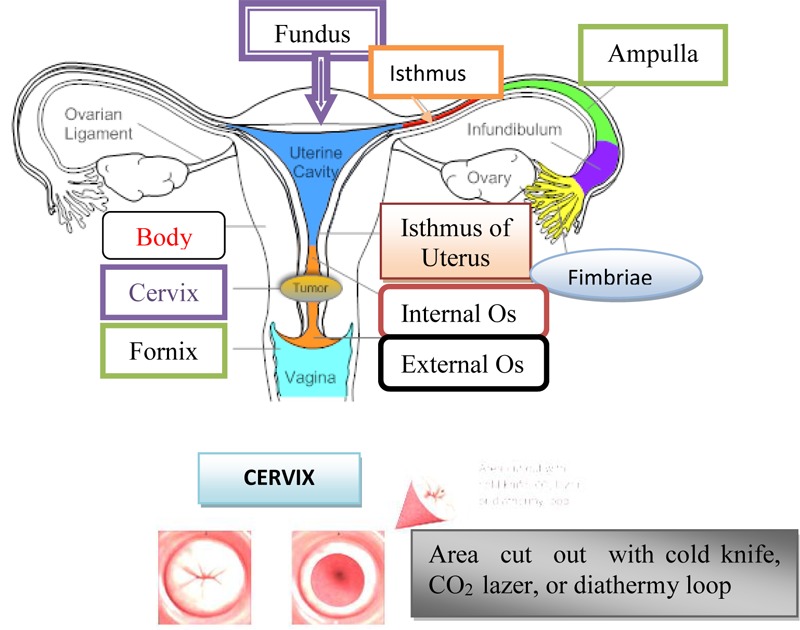
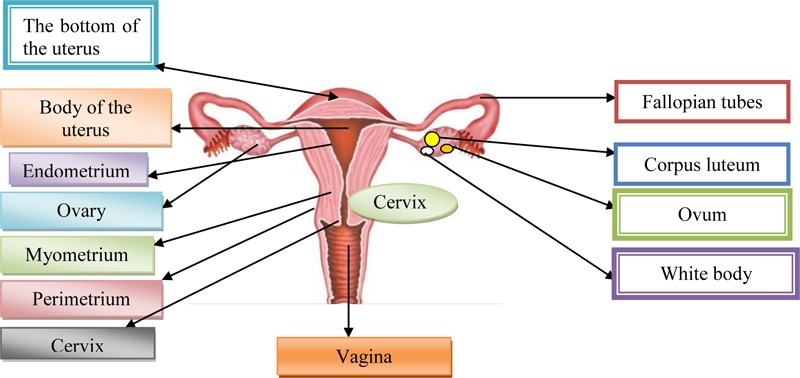
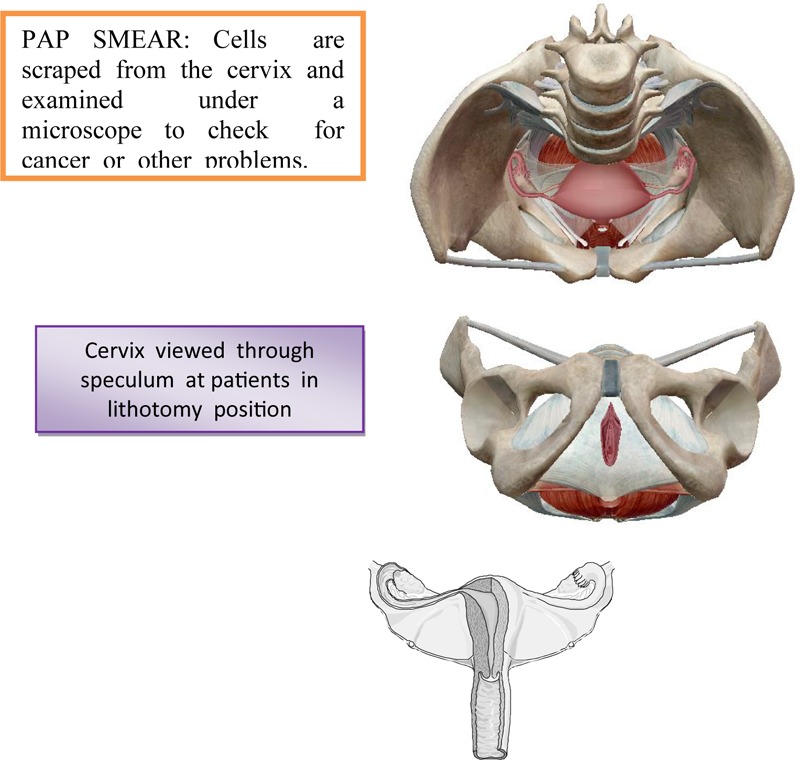
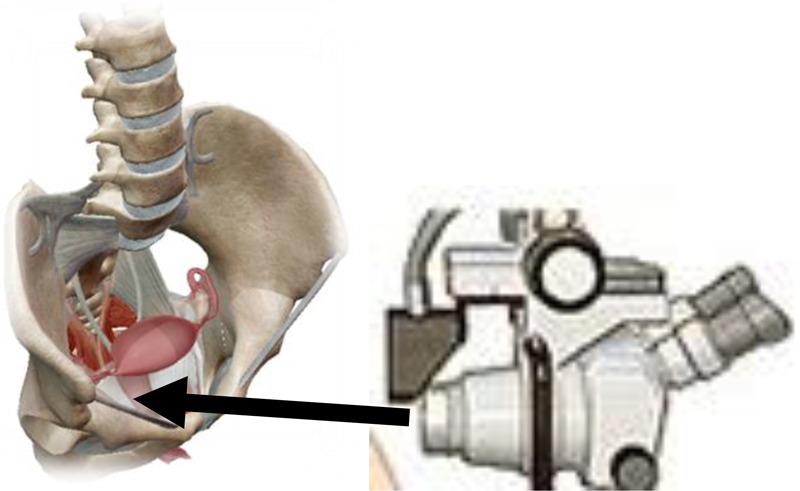
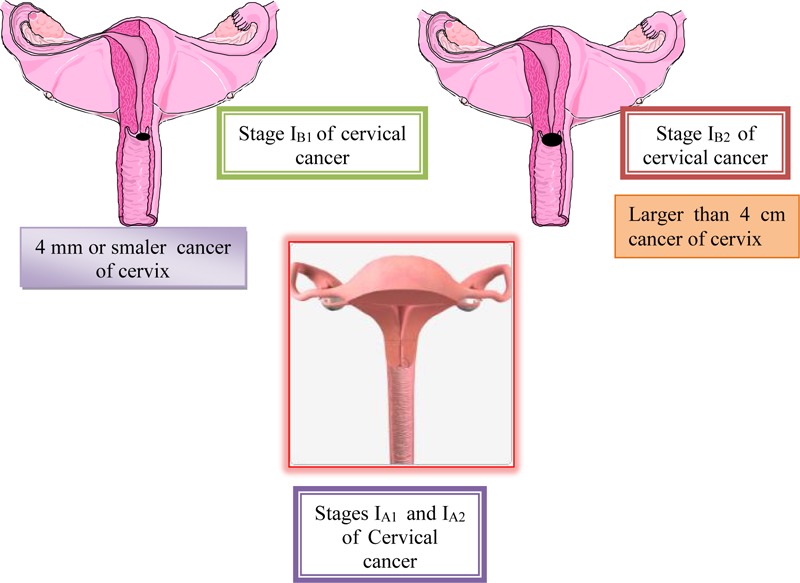
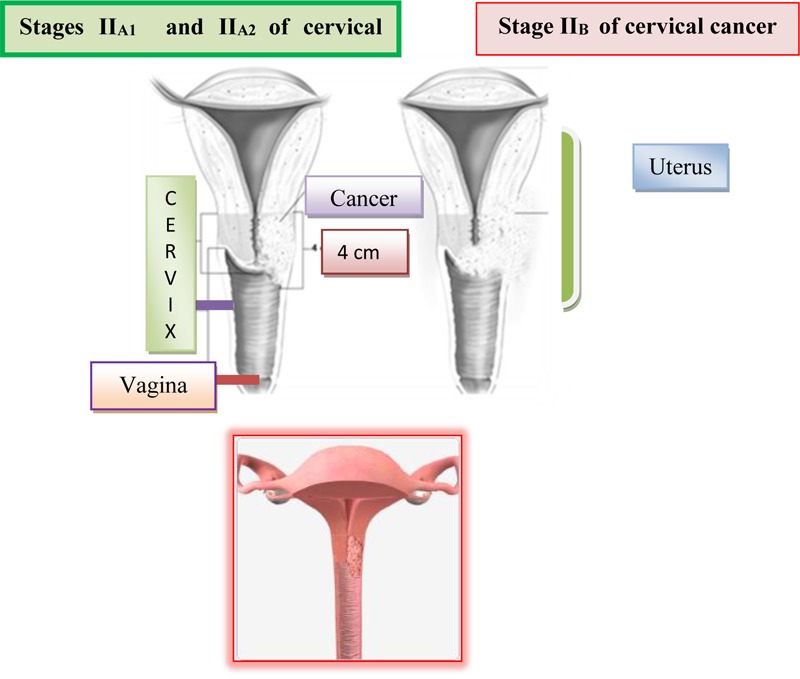
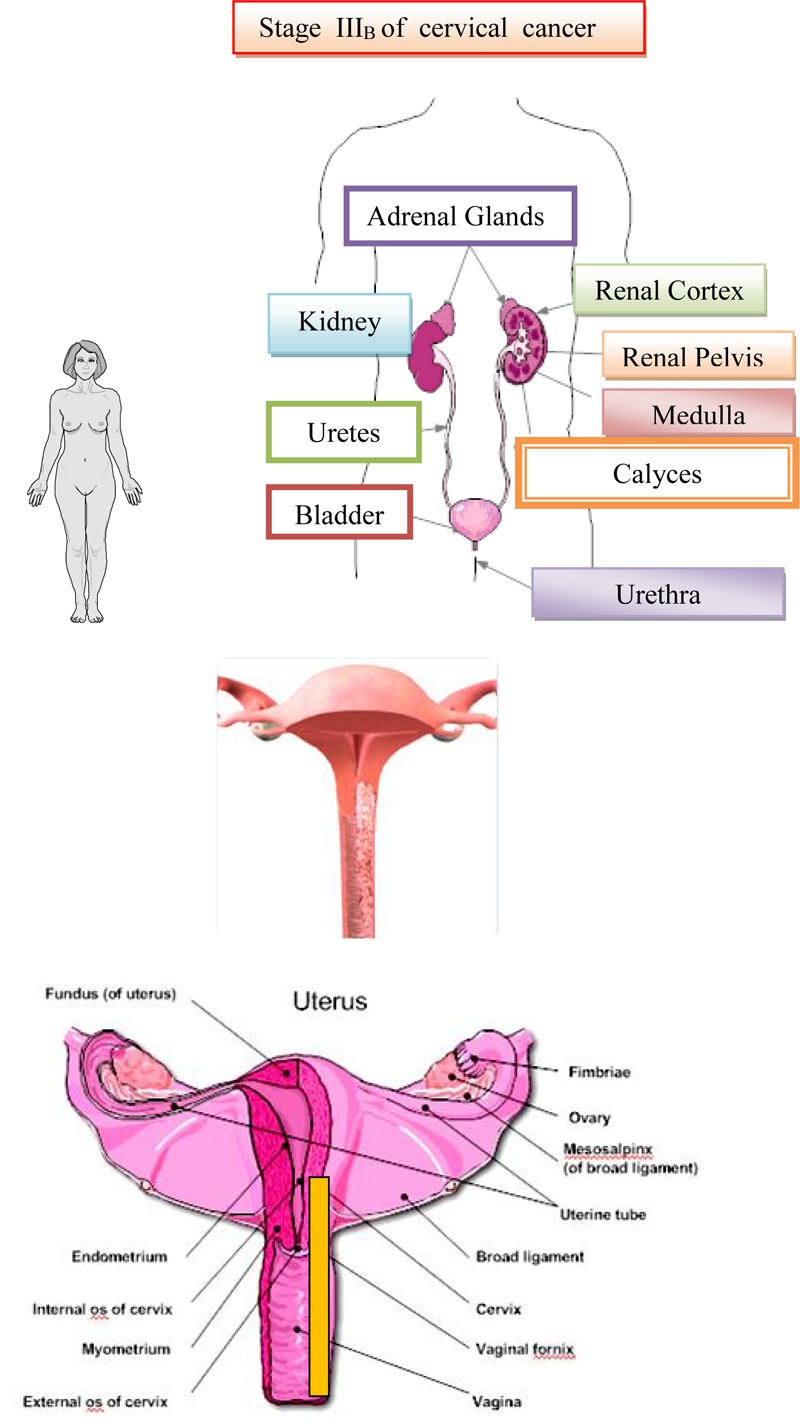
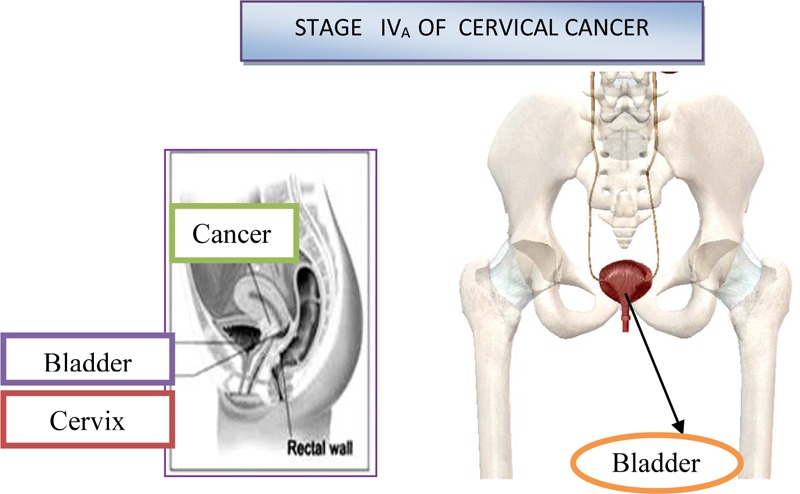
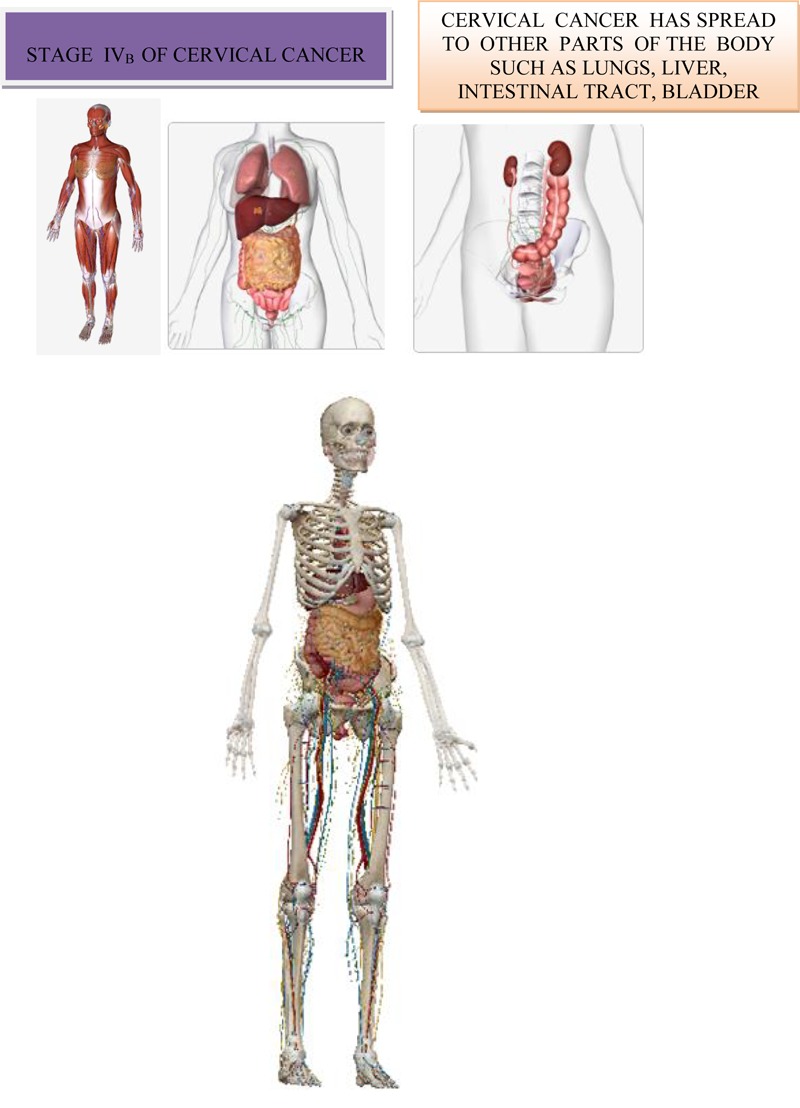
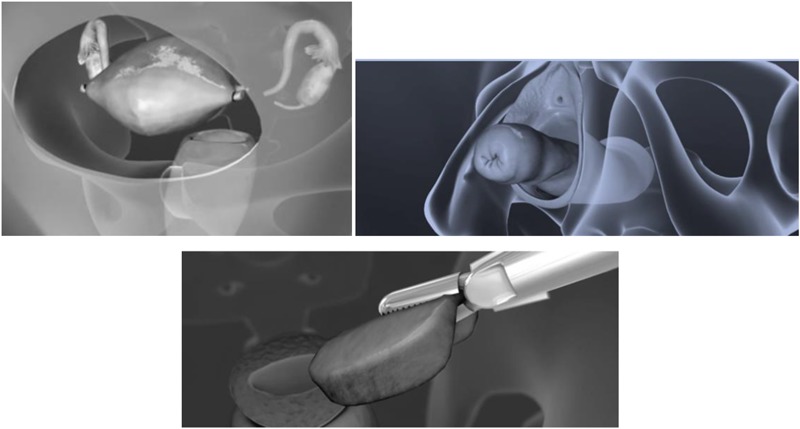
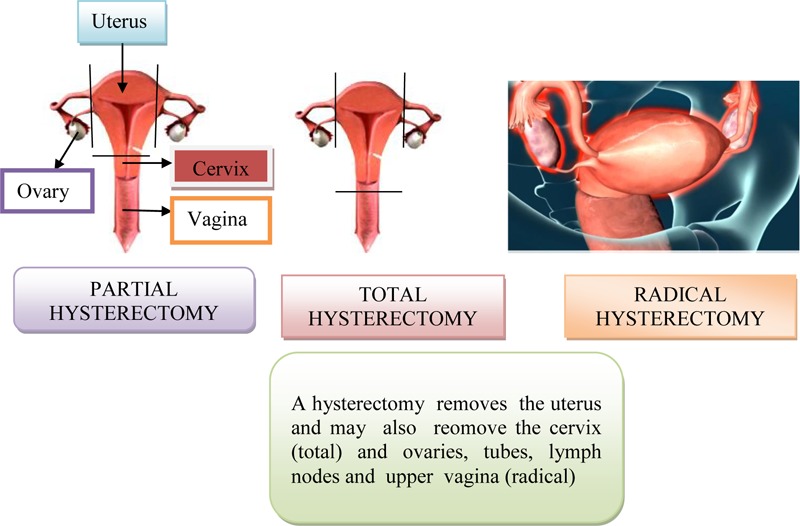
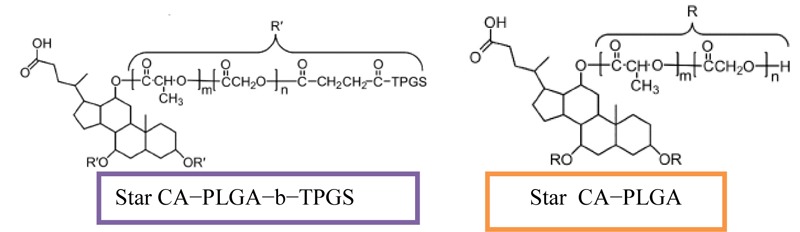
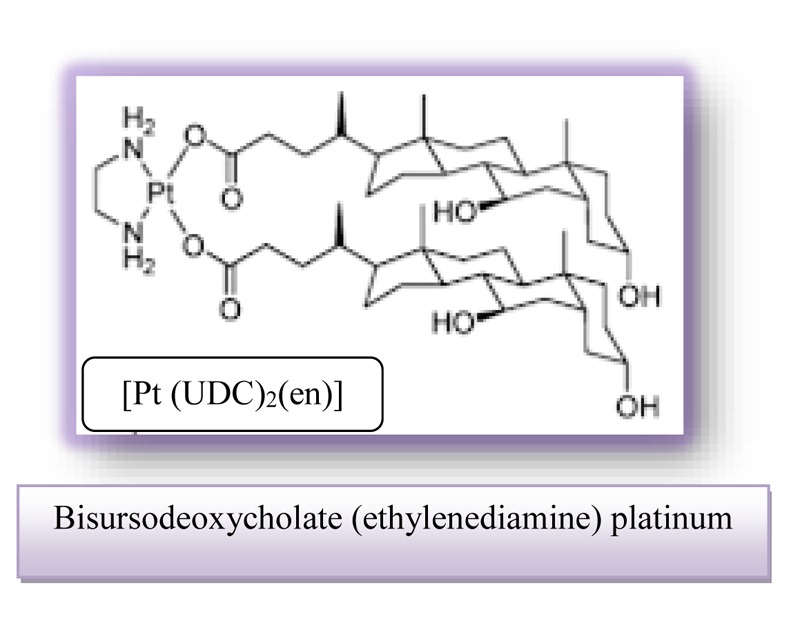
Cervical cancer can be cured, because it has a long preinvasive period. Early diagnosis and treatment of cervical cancer at women are crucial for reducing of rate mortality. Today, there are many methods for detecting premalignant lesions and one of them is a conventional Papanicolaou test. Cervical cancer develops through a series of changes in the epithelium called cervical intraepithelial neoplasia (CIN). The biological and genetic characteristics of the cells at cancer in situ are irreversibly altered and abnormal cells have the potential to metastasize to others anatomical regions. Infection with human Papillomavirus, which is transmitted sexually, is considered the main cause and represent the necessary, but not the only factor for the development of cervical cancer. Types of high risk human Papillomavirus are often associated with invasive cervical cancer. The carcinogenic types of HPV 16 and 18 are responsible for 70% of cervical cancer and about 50% of CIN 3. Primary prevention of cervical cancer is aimed at reducing incidence, control of causes and risk factors. In this scientific work, in addition to explaining the various treatments necessary for the treatment of cervical carcinoma, we were discussed about the anticancer effects of the synthetic derivative of ursodeoxycholic acid, such as HS-1183, and synthetic derivatives of chenodeoxycholic acid such as HS-1199 and HS-1200. Also, the effects of bile acid complexes with metals such as platinum, zinc, nickel, and copper were considered in the effective treatment of cervical cancer. KEY POINTS • Lymphogenic spreading of cervical cancer occurs relatively early in the regional lymph nodes, while this sort of progression of cervical cancer is rarer in the juxtaregional (paraaortic), mediastinal and supraclavicular nodes. Clinically proven supraclavicular metastases are not a rarity. In stages IIb and IIIa with metastases in paraaortal nodes occur a 20% metastases at the neck lymph nodes. Hematogenic metastases are relatively rare and occur in the posterior phase. Distant metastases are detected in the lungs and liver. Preinvasive and microinvasive stages of cervical cancer are without symptoms. With deeper invasion of the strome, certain clinical symptoms such as prolonged menstruation, increased vaginal secretions, vaginal bleeding between the two periods, contact bleeding (after coitus), unilateral pelvic pain with spreading in hip joint (infiltration of the pelvic nerve plexus), dysuric disturbance, anemia, islet of the lower extremities. In order to diagnose the level spreading of primary lesion of cervical cancer most commonly are used the supplemental searches such as cytoscopy, rectoscopy, urography, irigography, lung and bone radiography, scintigraphy of the liver, kidney and bone, lymphography, CT (MR) of abdomen and pelvis, as well as laboratory analysis. Surgical treatment consists of transvaginal hysterectomy, transabdominal removal of the uterus (via laparotomy), bilateral adenectomy (removal of the ovaries and the fallopian tubes), upper and middle third of the vagina and lymphonodectomy of the regional lymph nodes. The most commonly used radiotherapy, intracavitary brachytherapy, manual afterloading technique and remote afterloading techniques. The synthetic derivatives of ursodeoxycholic acid and chenodeoxycholic acid such as HS-1183, HS-1199, and HS-1200 are used to treat cervical cancer. These derivatives of chenodeoxycholic acid and ursodeoxycholic acid are capable of inhibiting cell proliferation and inducing apoptosis in SiHa human cells of cervix. Platinum compounds are used as catalysts in cervical cancer therapy. Clinical use of platinum complexes for which the bile acids bind is based on the desire to achieve the death of tumor cells and the spectrum of drug activity in the treatment of cervical cancer. Bisursodeoxycholate (ethylenediamine) platinum (II) [Pt(UDC)2(en)] is characterized by important cytotoxicity against HeLa cervical carcinoma cells and this effect already being clearly detectable after 24 h.
Keywords: bile acids; cervical cancer; different treatments; therapeutic agents; treatment of cervical cancer.
Figures


References
-
- American Joint Committee on Cancer [AJCC] (2017). Cervix Uteri in AJCC Cancer Staging Manual 8th Edn. New York, NY: Springer; 649–659.
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials