

The High Prevalence of Testicular Adrenal Rest Tumors in Adult Men With Congenital Adrenal Hyperplasia Is Correlated With ACTH Levels
- PMID: 31214118
- PMCID: PMC6558150
- DOI: 10.3389/fendo.2019.00335
The High Prevalence of Testicular Adrenal Rest Tumors in Adult Men With Congenital Adrenal Hyperplasia Is Correlated With ACTH Levels
Abstract
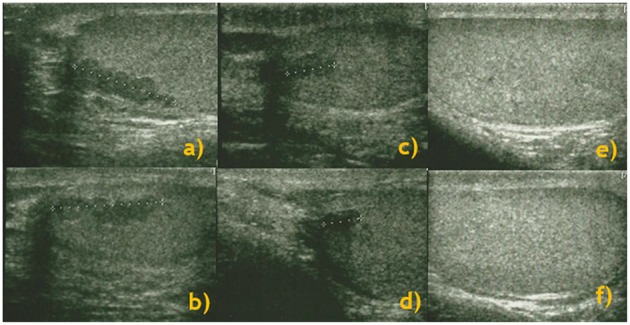
Introduction: The aims of this study were to determine the prevalence of testicular-adrenal rest tumors (T-ARTs) in patients with congenital adrenal hyperplasia (CAH) and to evaluate the related ultrasound (US) features, hormonal profiles, and semen parameters. Therefore, we attempted to understand the potential impact of adrenocorticotropic hormone (ACTH) on the persistence or disappearance of T-ART. Methods: We conducted a longitudinal cohort study including patients with CAH who were undergoing treatment with cortisone and, when indicated, fludrocortisone replacement therapy. We performed andrological examinations, US of the testis, hormone profiling, and semen analysis. Results: Of the 25 patients (mean ± SD age, 32.2 ± 7.5 years), T-ARTs were detected by US in 14 (56.0%) patients. The mean ± SD diameter of the lesions was 13.2 ± 6.8 mm. Among 3 (21.4%) patients, the lesions were observed in one testis, whereas both testes were affected in the remaining 11 (78.6%) patients. The lesions were hypoechoic in 12 (85.7%) patients and hyperechoic in 2 (14.3%). Plasma ACTH and 17-hydroxyprogesterone (17-OHP) levels were significantly higher in patients with T-ART than in patients without lesions (319.4 ± 307.0 pg/ml and 12.4 ± 2.7 ng/ml vs. 33.5 ± 10.7 pg/ml and 8.2 ± 1.8 ng/ml, respectively; p < 0.01). The mean values of sperm concentration and motility were significantly lower in patients with T-ART than in patients without lesions (12.1 ± 12.4 × 106 cells/ml and 18.4 ± 11.1% vs. 41.5 ± 23.2 × 106 cells/ml and 30.8 ± 15.4%, respectively; p < 0.05). Logistic regression analysis showed ACTH level as a significant predictor of T-ART (p < 0.05). In patients with T-ART, the dose of hydrocortisone was increased by ~25-30%, while the fludrocortisone treatment remained unchanged. After 6 months of steroid treatment, patients underwent US and hormonal evaluation. Disappearance and a reduction in T-ART were observed in 6 (42.9%) and 5 (35.7%) patients, respectively; a reduction in ACTH levels (from 319.4 ± 307.0 to 48.1 ± 5.1 pg/ml; p < 0.01) was reported. A significant correlation between ACTH level reduction and T-ART diameter reduction was observed (p < 0.5; r = 0.55). Conclusions: T-ARTs were detected in 56% of patients with CAH and were associated with impaired semen parameters. However, these lesions are potentially reversible, as demonstrated by the disappearance/reduction after adjustment of cortisone therapy and by the reduction in plasma ACTH level. Our study supports the importance of periodic US evaluation and maintenance of plasma ACTH levels within the normal range in men with CAH.
Keywords: azoospermia; congenital adrenal hyperplasia; cortisol; male infertility; semen analysis; testicular adrenal rest tumor; testicular lesion; testosterone.
Figures
Similar articles
-
Sonographic features of the testicular adrenal rests tumors in patients with congenital adrenal hyperplasia: a single-center experience and literature review.Orphanet J Rare Dis. 2019 Nov 6;14(1):242. doi: 10.1186/s13023-019-1231-1. Orphanet J Rare Dis. 2019. PMID: 31694673 Free PMC article. Review.
-
Testicular adrenal rest tumors in patients with congenital adrenal hyperplasia: prevalence and sonographic, hormonal, and seminal characteristics.J Ultrasound Med. 2012 Mar;31(3):383-8. doi: 10.7863/jum.2012.31.3.383. J Ultrasound Med. 2012. PMID: 22368128
-
Restoration of fertility by gonadotropin replacement in a man with hypogonadotropic azoospermia and testicular adrenal rest tumors due to untreated simple virilizing congenital adrenal hyperplasia.Eur J Endocrinol. 2014 Mar 13;170(4):K11-7. doi: 10.1530/EJE-13-0449. Print 2014 Apr. Eur J Endocrinol. 2014. PMID: 24394723
-
Classical congenital adrenal hyperplasia due to 21-hydroxylase deficiency (21-OHD) in adult males: Clinical presentation, hormone function and the detection of adrenal and testicular adrenal rest tumors (TARTs).Endocrinol Diabetes Nutr (Engl Ed). 2021 Apr;68(4):227-235. doi: 10.1016/j.endien.2020.07.003. Endocrinol Diabetes Nutr (Engl Ed). 2021. PMID: 34266634
-
Testicular adrenal rest tumors - Epidemiology, diagnosis and treatment.J Pediatr Urol. 2024 Feb;20(1):77-87. doi: 10.1016/j.jpurol.2023.10.005. Epub 2023 Oct 7. J Pediatr Urol. 2024. PMID: 37845103 Review.
Cited by
-
Scrotal Ultrasonography Features of Testicular Adrenal Rest Tumors in Male Congenital Adrenal Hyperplasia Patients: A Systematic Review.Indian J Endocrinol Metab. 2025 Mar-Apr;29(2):133-141. doi: 10.4103/ijem.ijem_19_24. Epub 2025 Apr 29. Indian J Endocrinol Metab. 2025. PMID: 40416457 Free PMC article. Review.
-
Sonographic features of the testicular adrenal rests tumors in patients with congenital adrenal hyperplasia: a single-center experience and literature review.Orphanet J Rare Dis. 2019 Nov 6;14(1):242. doi: 10.1186/s13023-019-1231-1. Orphanet J Rare Dis. 2019. PMID: 31694673 Free PMC article. Review.
-
Morphologic and Molecular Characterization of Adrenals and Adrenal Rest Affected by Congenital Adrenal Hyperplasia.Front Endocrinol (Lausanne). 2021 Sep 20;12:730947. doi: 10.3389/fendo.2021.730947. eCollection 2021. Front Endocrinol (Lausanne). 2021. PMID: 34616364 Free PMC article.
-
Congenital Adrenal Hyperplasia-Current Insights in Pathophysiology, Diagnostics, and Management.Endocr Rev. 2022 Jan 12;43(1):91-159. doi: 10.1210/endrev/bnab016. Endocr Rev. 2022. PMID: 33961029 Free PMC article. Review.
-
Erectile Dysfunction Severity: The Role of Glycometabolic Compensation and Antihyperglycemic Drugs.J Clin Med. 2022 Dec 5;11(23):7214. doi: 10.3390/jcm11237214. J Clin Med. 2022. PMID: 36498788 Free PMC article.
References
-
- Mass Screening Committee Japanese Society for Pediatric Endocrinology and Japanese Society for Mass Screening. Ishii T, Anzo M, Adachi M, Onigata K, Kusuda S, et al. . Guidelines for diagnosis and treatment of 21-hydroxylase deficiency (2014 revision). Clin Pediatr Endocrinol. (2015) 24:77–105. 10.1297/cpe.24.77 - DOI - PMC - PubMed
-
- Speiser PW, Azziz R, Baskin LS, Ghizzoni L, Hensle TW, Merke DP, et al. . Endocrine Society: congenital adrenal hyperplasia due to steroid 21-hydroxylase deficiency: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. (2010) 95:4133–60. 10.1210/jc.2009-2631 - DOI - PMC - PubMed
-
- Stikkelbroeck NM, Otten BJ, Pasic A, Jager GJ, Sweep CG, Noordam K, et al. . High prevalence of testicular adrenal rest tumors, impaired spermatogenesis, and Leydig cell failure in adolescent and adult males with congenital adrenal hyperplasia. J. Clin. Endocrinol. Metab. (2001) 86:5721–8. 10.1210/jcem.86.12.8090 - DOI - PubMed
LinkOut - more resources
Full Text Sources