

Laparoscopic Surgery for Gastric Cancer: The European Point of View
- PMID: 31214260
- PMCID: PMC6535846
- DOI: 10.1155/2019/8738502
Laparoscopic Surgery for Gastric Cancer: The European Point of View
Abstract
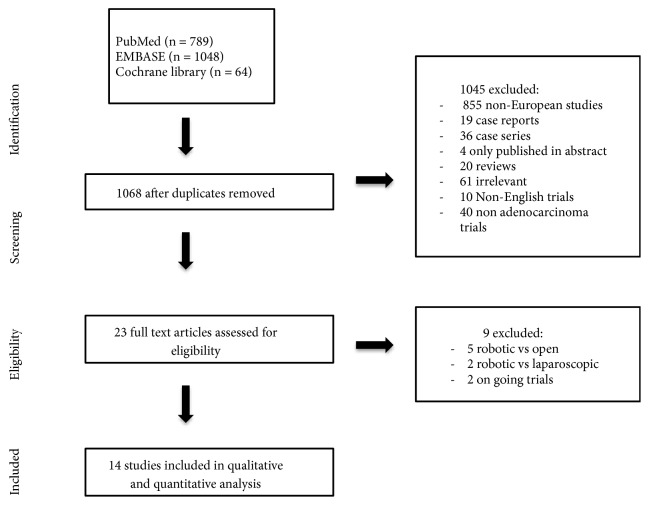
Objective: Multiple Asian studies have proved the feasibility of laparoscopic approach for surgical treatment of gastric cancer. The difference between Asian and European patients could limit their application in Europe. We reviewed the literature for European studies comparing open gastrectomy with laparoscopic approach in the treatment of gastric cancer.
Method: We searched the keywords gastric cancer and laparoscopy in MEDLINE and EMBASE. We included all studies published between 1990 and 2016 and conducted in Europe.
Result: We found 1 randomized and 13 cohort studies which compared laparoscopic with open gastrectomy. We found no mean difference in the number of lymph nodes harvested between laparoscopic and open group (mean difference: -0.49; 95% CI: -2.42; 1.44, p=0.62) and no difference of short-term or long-term mortality (short-term odds ratio: 0.74, p=0.47; long-term odds ratio: 0.65, p=0.11). We found a longer operative time in the laparoscopic group (mean difference: 35.75 minutes, p<0.01) but lesser reoperation rate than the open group (odds ratio: 1.55 p=0.01).
Conclusion: European based population studies found results comparable with their Asian counterpart. In the current state of evidence, minimally invasive surgery for gastric cancer is safe and can achieve the same oncological results.
Figures



References
-
- Japanese Gastric Cancer Association. Japanese gastric cancer treatment guidelines 2010. Gastric Cancer. 2011;14(2):113–123. - PubMed
-
- Guillou P. J., Quirke P., Thorpe H., et al. Short-term endpoints of conventional versus laparoscopic-assisted surgery in patients with colorectal cancer (MRC CLASICC trial): multicentre, randomised controlled trial. The Lancet. 2005;365(9472):1718–1726. doi: 10.1016/s0140-6736(05)66545-2. - DOI - PubMed
-
- Kitano S., Iso Y., Moriyama M., et al. Laparoscopy-assisted Billroth I gastrectomy. Surgical Laparoscopy Endoscopy. 1994;4:146–148. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
