

Tumor Enucleation vs. Partial Nephrectomy for T1 Renal Cell Carcinoma: A Systematic Review and Meta-Analysis
- PMID: 31214511
- PMCID: PMC6557988
- DOI: 10.3389/fonc.2019.00473
Tumor Enucleation vs. Partial Nephrectomy for T1 Renal Cell Carcinoma: A Systematic Review and Meta-Analysis
Abstract
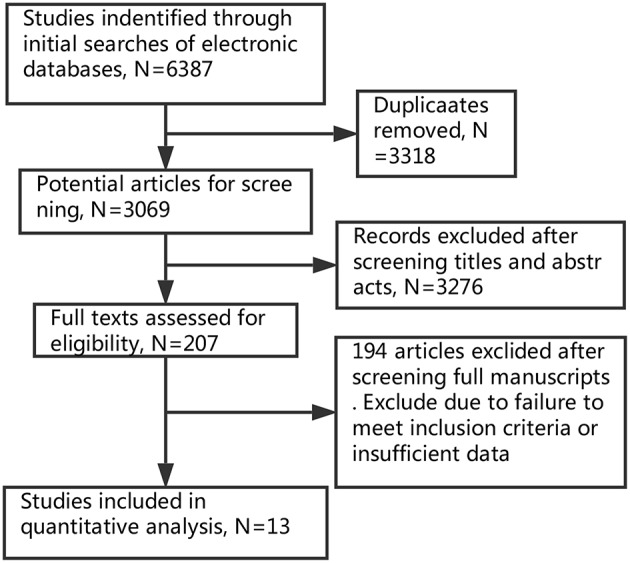
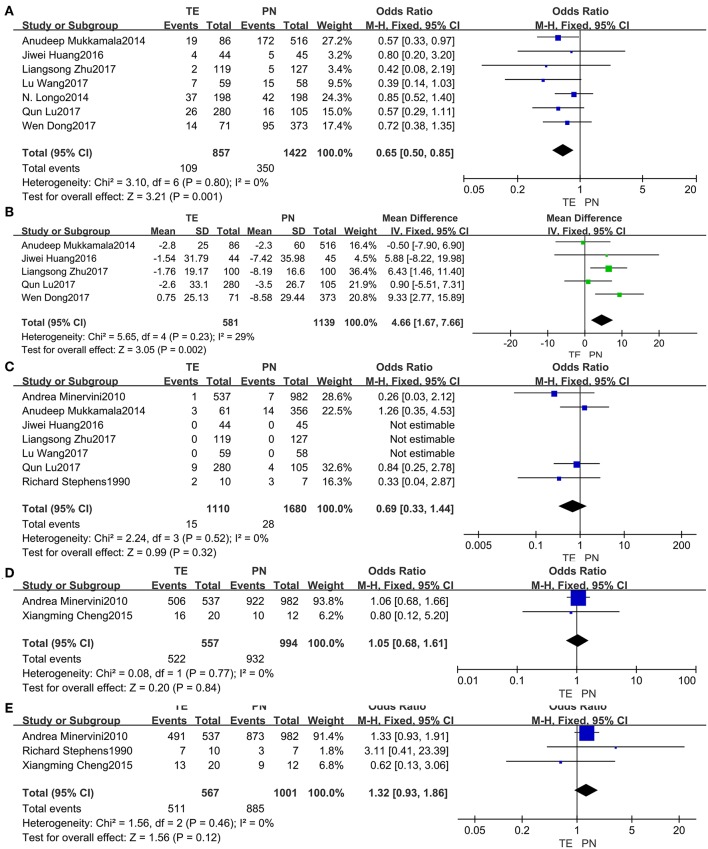
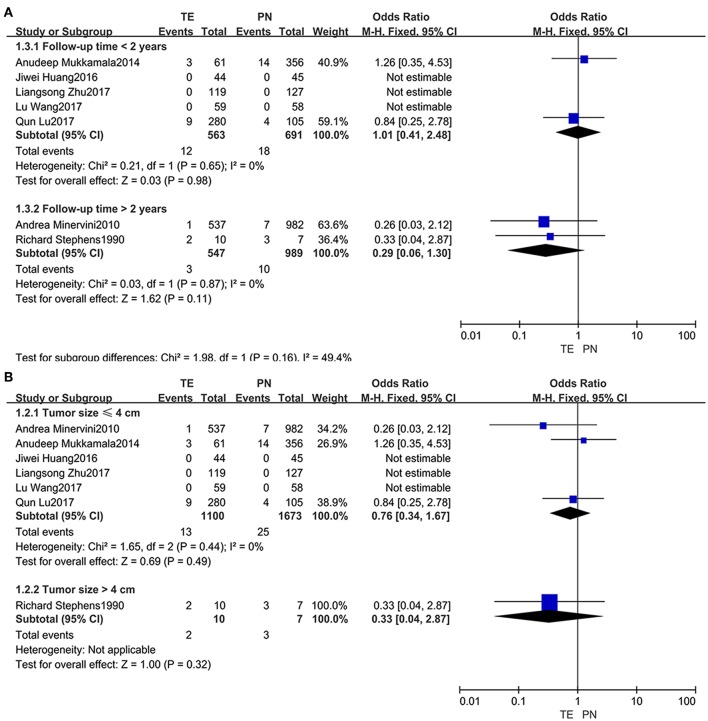
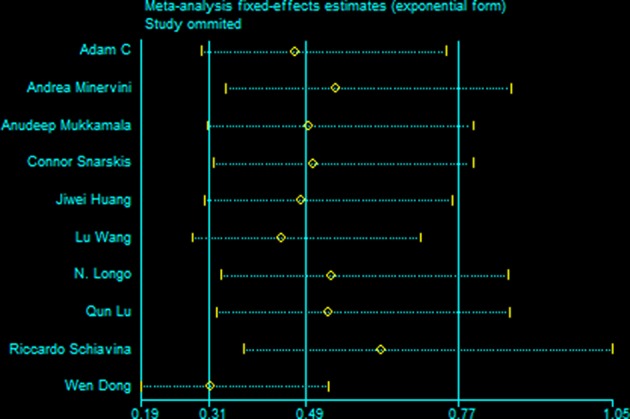
Purpose: Tumor enucleation (TE) and partial nephrectomy (PN) have both become main treatment strategies for T1 renal cell carcinoma (RCC), despite the discrepancy between their safety margin. We performed a meta-analysis on all the relevant trials in order to compare the clinical efficacy and safety of TE with those of PN for RCC treatment. Methods: In this meta-analysis, randomized controlled trials or retrospective studies were included if they compared TE and PN therapy in patients with localized renal cancer. The main outcomes extracted were perioperative data and post-operative outcomes. Subgroups for analyses were undertaken according to tumor size and duration of follow up. Data were pooled using the generic variance method with a fixed or random effects model and expressed as mean differences or odds ratios with 95% CI. Results: A total of 13 studies containing 1,792 patients undergoing TE and 3,068 undergoing PN were identified. Our study showed that the patients received TE had significantly shorter operative time (MD = -28.46, 95% CI = -42.09, -14.83, P < 0.0001), less hospital day (MD = -0.68, 95% CI = -1.04, -0.31, P = 0.0003), less estimate blood loss (MD = -59.90, 95% CI = -93.23, -26.58, P = 0.0004) and smaller change in estimated glomerular filtration rate (fixed effect: MD = 4.66, 95% CI = 1.67, 7.66, P = 0.002), fewer complications (fixed effect: OR = 0.65, 95% CI = 0.50, 0.85, P = 0.001) compared with those received PN. However, there were no significant differences in terms of warm ischemic time, positive margin rates, recurrence rates and survival rates between the two groups. All the subgroup analyses presented consistent results with the overall analyses. Conclusions: Our findings suggested that TE is not only less-traumatizing and beneficial for recovery, but also better for renal function protection. Moreover, it did not show the evidence of an increase relapse rate or mortality rate when compared with PN.
Keywords: meta-analysis; nephron sparing surgery; partial nephrectomy; renal cell carcinoma; tumor enucleation.
Figures

Similar articles
-
Partial nephrectomy versus radical nephrectomy for large (≥ 7 cm) renal tumors: A systematic review and meta-analysis.Urol Oncol. 2019 Apr;37(4):263-272. doi: 10.1016/j.urolonc.2018.12.015. Epub 2019 Jan 28. Urol Oncol. 2019. PMID: 30704957
-
Comparison of Sutureless Versus Suture Partial Nephrectomy for Clinical T1 Renal Cell Carcinoma: A Meta-Analysis of Retrospective Studies.Front Oncol. 2021 Sep 2;11:713645. doi: 10.3389/fonc.2021.713645. eCollection 2021. Front Oncol. 2021. PMID: 34540681 Free PMC article.
-
Robotic partial nephrectomy with superselective versus main artery clamping: a retrospective comparison.Eur Urol. 2014 Oct;66(4):713-9. doi: 10.1016/j.eururo.2014.01.017. Epub 2014 Jan 25. Eur Urol. 2014. PMID: 24486306
-
Tumor enucleation specimens of small renal tumors more frequently have a positive surgical margin than partial nephrectomy specimens, but this is not associated with local tumor recurrence.Virchows Arch. 2017 Jan;470(1):55-61. doi: 10.1007/s00428-016-2031-9. Epub 2016 Oct 24. Virchows Arch. 2017. PMID: 27778094
-
Robotic unclamped "minimal-margin" partial nephrectomy: ongoing refinement of the anatomic zero-ischemia concept.Eur Urol. 2015 Oct;68(4):705-12. doi: 10.1016/j.eururo.2015.04.044. Epub 2015 Jun 11. Eur Urol. 2015. PMID: 26071789
Cited by
-
Tumor enucleation for the treatment of T1 renal tumors: A systematic review and meta-analysis.Investig Clin Urol. 2022 Mar;63(2):126-139. doi: 10.4111/icu.20210361. Investig Clin Urol. 2022. PMID: 35244986 Free PMC article.
-
X-Capsular Incision for Tumor Enucleation (X-CITE)-Technique: A Method to Maximize Renal Parenchymal Preservation for Completely Endophytic Renal Tumors.Urology. 2021 Aug;154:315-319. doi: 10.1016/j.urology.2021.03.032. Epub 2021 Apr 5. Urology. 2021. PMID: 33831400 Free PMC article.
-
The Benign Renal Masses that Were Exposed after Nephron-Sparing Surgery: "Postsurgical Fatty Tumor." Is It Related to the Surgical Technique?J Kidney Cancer VHL. 2021 Nov 28;9(1):1-8. doi: 10.15586/jkcvhl.v9i1.195. eCollection 2022. J Kidney Cancer VHL. 2021. PMID: 34888127 Free PMC article.
-
Visualization modality for augmented reality guidance of in-depth tumour enucleation procedures.Healthc Technol Lett. 2023 Dec 3;11(2-3):101-107. doi: 10.1049/htl2.12058. eCollection 2024 Apr-Jun. Healthc Technol Lett. 2023. PMID: 38638490 Free PMC article.
-
A Hemostatic Technique in Robot-Assisted Laparoscopic Partial Nephrectomy and Its Impact on Renal Function.Cureus. 2021 May 19;13(5):e15122. doi: 10.7759/cureus.15122. Cureus. 2021. PMID: 34159024 Free PMC article.
References
-
- Huang J, Zhang J, Wang Y, Kong W, Xue W, Liu D, et al. . Comparing zero ischemia laparoscopic radio frequency ablation assisted tumor enucleation and laparoscopic partial nephrectomy for clinical T1a renal tumor: a randomized clinical trial. J Urol. (2016) 195:1677–83. 10.1016/j.juro.2015.12.115 - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources