

Reduced Transplacental Transfer of Antimalarial Antibodies in Kenyan HIV-Exposed Uninfected Infants
- PMID: 31214627
- PMCID: PMC6563943
- DOI: 10.1093/ofid/ofz237
Reduced Transplacental Transfer of Antimalarial Antibodies in Kenyan HIV-Exposed Uninfected Infants
Abstract
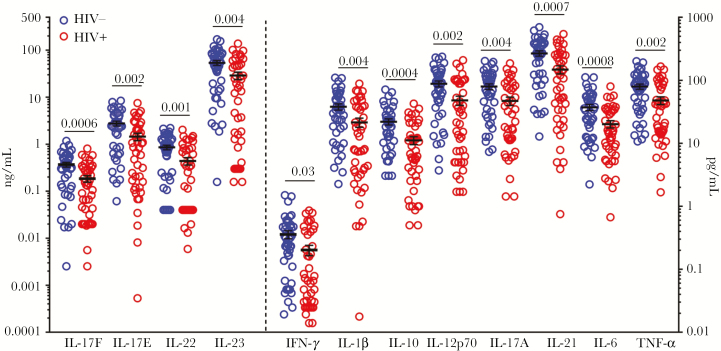
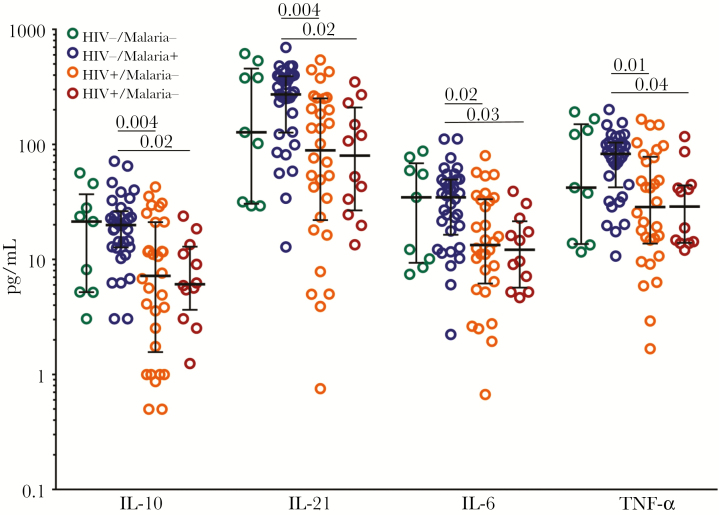
Background: Altered neonatal immune responses may contribute to the increased morbidity observed in HIV-exposed but uninfected (HEU) infants compared with HIV-unexposed uninfected (HUU) infants. We sought to examine the effects of prenatal HIV and malaria exposure on maternal and neonatal plasma cytokine profiles and transplacental antibody transfer.
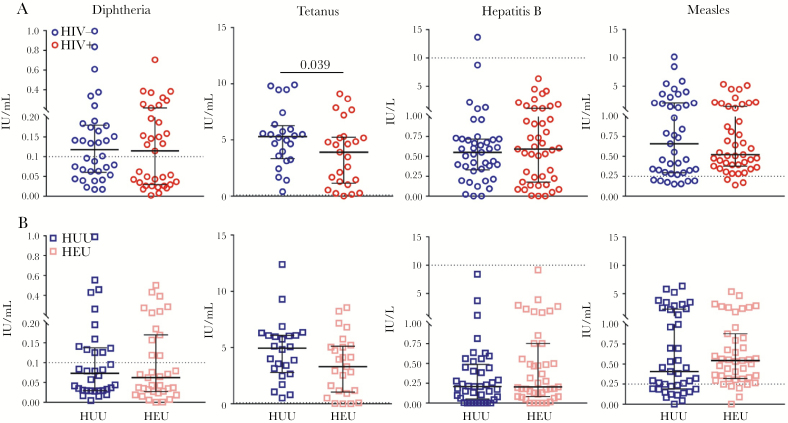
Methods: Forty-nine HIV+ and 50 HIV- women and their HIV-uninfected neonate pairs from Kenya were assessed. All HIV+ mothers received combination antiretroviral therapy. Maternal plasma and cord blood plasma samples at delivery were tested for 12 cytokines, total IgG, and IgG specific to 4 vaccine antigens and 14 Plasmodium falciparum antigens.
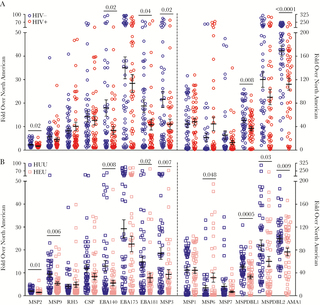
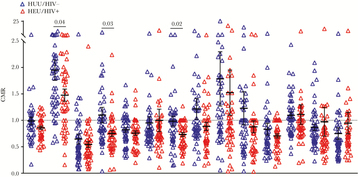
Results: HIV+ mothers had lower levels of all 12 plasma cytokines at delivery compared with HIV- mothers, but there were no differences between HEU and HUU neonates. There were no differences in the cord-to-maternal ratios (CMRs) of vaccine-specific IgG between HIV+/HEU and HIV-/HUU maternal-neonate pairs. HIV+/HEU maternal-neonate pairs had significantly lower CMRs for 3 antimalarial IgGs-merozoite surface protein 9, circumsporozoite protein, and erythrocyte binding antigen 181-which remained statistically significant after adjustment for malaria in pregnancy.
Conclusions: In a cohort of optimally treated HIV-infected pregnant women, maternal HIV infection was associated with reduced transplacental transfer of antimalarial antibodies.
Keywords: HIV-exposed uninfected neonate; antimalarial antibodies; inflammation; malaria; transplacental antibody transfer; vaccines.
Figures
References
-
- Wedi CO, Kirtley S, Hopewell S, et al. . Perinatal outcomes associated with maternal HIV infection: a systematic review and meta-analysis. Lancet HIV 2016; 3:e33–48. - PubMed
-
- Okoko BJ, Enwere G, Ota MO. The epidemiology and consequences of maternal malaria: a review of immunological basis. Acta Trop 2003; 87:193–205. - PubMed
-
- Klement E, Pitché P, Kendjo E, et al. . Effectiveness of co-trimoxazole to prevent Plasmodium falciparum malaria in HIV-positive pregnant women in sub-Saharan Africa: an open-label, randomized controlled trial. Clin Infect Dis 2014; 58:651–9. - PubMed
-
- UNAIDS. Data 2018. Geneva, Switzerland: Joint United Nations Programme on HIV/AIDS (UNAIDS); 2018. - PubMed
-
- Marinda E, Humphrey JH, Iliff PJ, et al. . ZVITAMBO Study Group Child mortality according to maternal and infant HIV status in Zimbabwe. Pediatr Infect Dis J 2007; 26:519–26. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
