

Columnar Injection for Intracerebral Cell Therapy
- PMID: 31214702
- PMCID: PMC7311830
- DOI: 10.1093/ons/opz143
Columnar Injection for Intracerebral Cell Therapy
Abstract
Background: Surgical implantation of cellular grafts into the brain is of increasing importance, as stem cell-based therapies for Parkinson and other diseases continue to develop. The effect of grafting technique on development and survival of the graft has received less attention. Rate and method of graft delivery may impact the cell viability and success of these therapies. Understanding the final location of the graft with respect to the intended target location is also critical.
Objective: To describe a "columnar injection" technique designed to reduce damage to host tissue and result in a column of graft material with greater surface area to volume ratio than traditional injection techniques.
Methods: Using a clinically relevant model system of human embryonic stem cell-derived dopaminergic progenitors injected into athymic rat host brain, we describe a novel device that allows separate control of syringe barrel and plunger, permitting precise deposition of the contents into the cannula tract during withdrawal. Controls consist of contralateral injection using traditional techniques. Graft histology was examined at graft maturity.
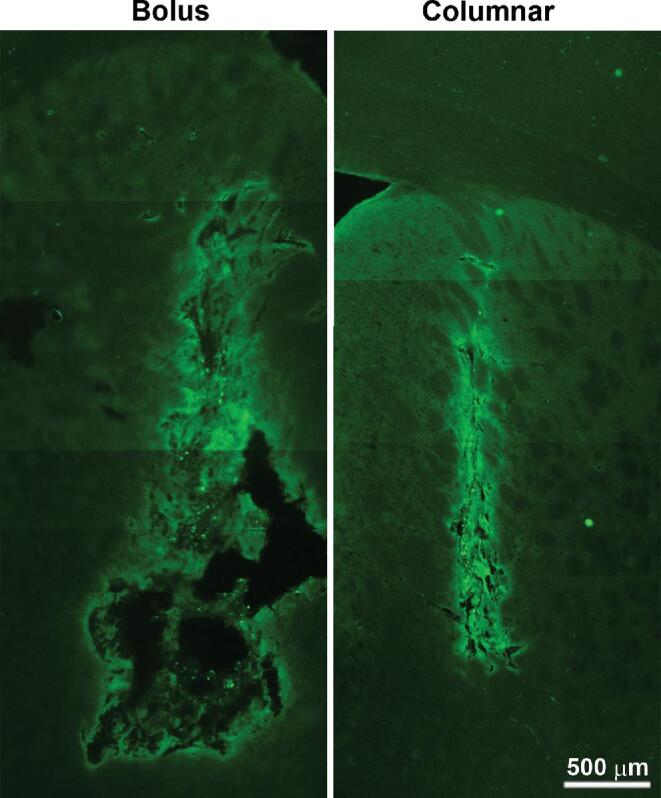
Results: Bolus grafts were centered on the injection tract but were largely proximal to the "target" location. These grafts displayed a conspicuous peripheral distribution of cells, particularly of mature dopaminergic neurons. In contrast, column injections remained centered at the intended target, contained more evenly distributed cells, and had significantly more mature dopaminergic neurons.
Conclusion: We suggest that this columnar injection technique may allow better engraftment and development of intracerebral grafts, enhancing outcomes of cell therapy, compared to fixed-point injection techniques.
Keywords: Cell therapy; Dopaminergic neurons; Stereotaxy.
Copyright © 2019 by the Congress of Neurological Surgeons.
Figures





References
-
- Backlund EO, Granberg PO, Hamberger Bet al.. Transplantation of adrenal medullary tissue to striatum in parkinsonism. First clinical trials. Proc Natl Acad Sci USA. 1985;62(2):1223-1232. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
