

Treatment Outcomes of Immune-Related Cutaneous Adverse Events
- PMID: 31216228
- PMCID: PMC7001790
- DOI: 10.1200/JCO.18.02141
Treatment Outcomes of Immune-Related Cutaneous Adverse Events
Abstract
Purpose: The aim of the current study was to report the efficacy of topical and systemic treatments for immune-related cutaneous adverse events (ircAEs) attributed to checkpoint inhibitors in an uncontrolled cohort of patients referred to oncodermatology clinics.
Methods: A retrospective analysis of patients with ircAEs evaluated by dermatologists from January 1, 2014, to December 31, 2017, at three tertiary care hospitals and cancer centers were identified through electronic medical records. Clinicopathologic characteristics, dermatologic therapy outcome, and laboratory data were analyzed.
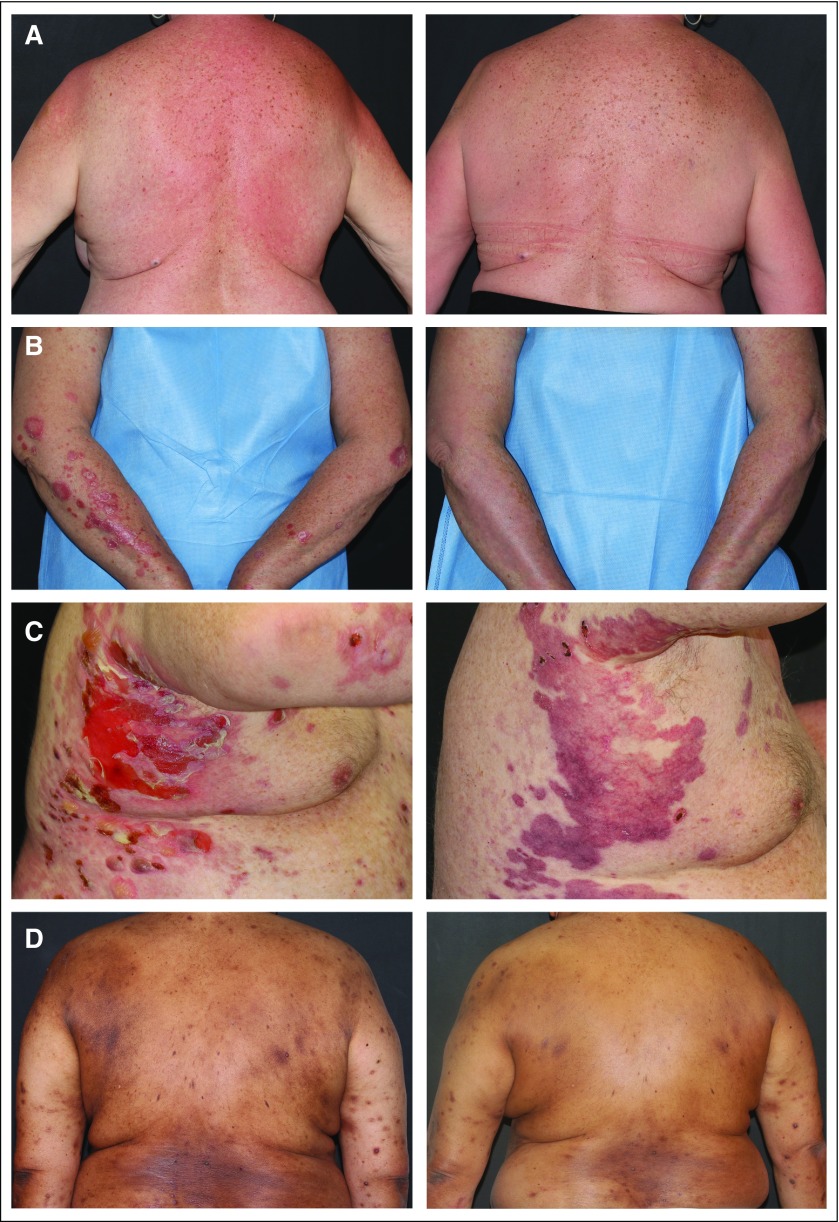
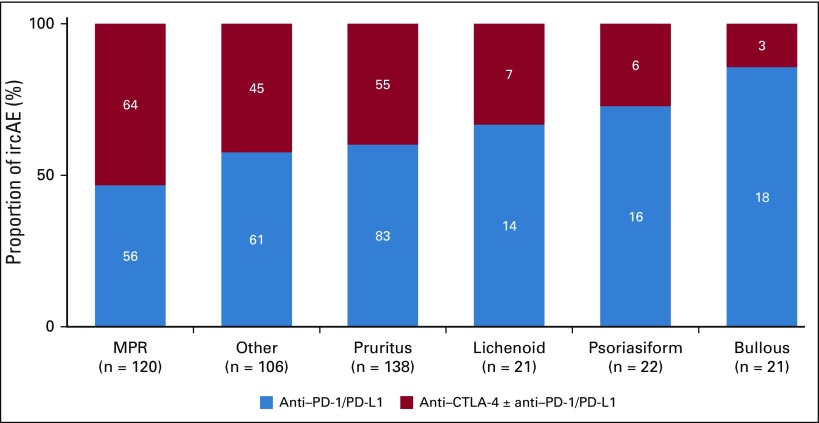
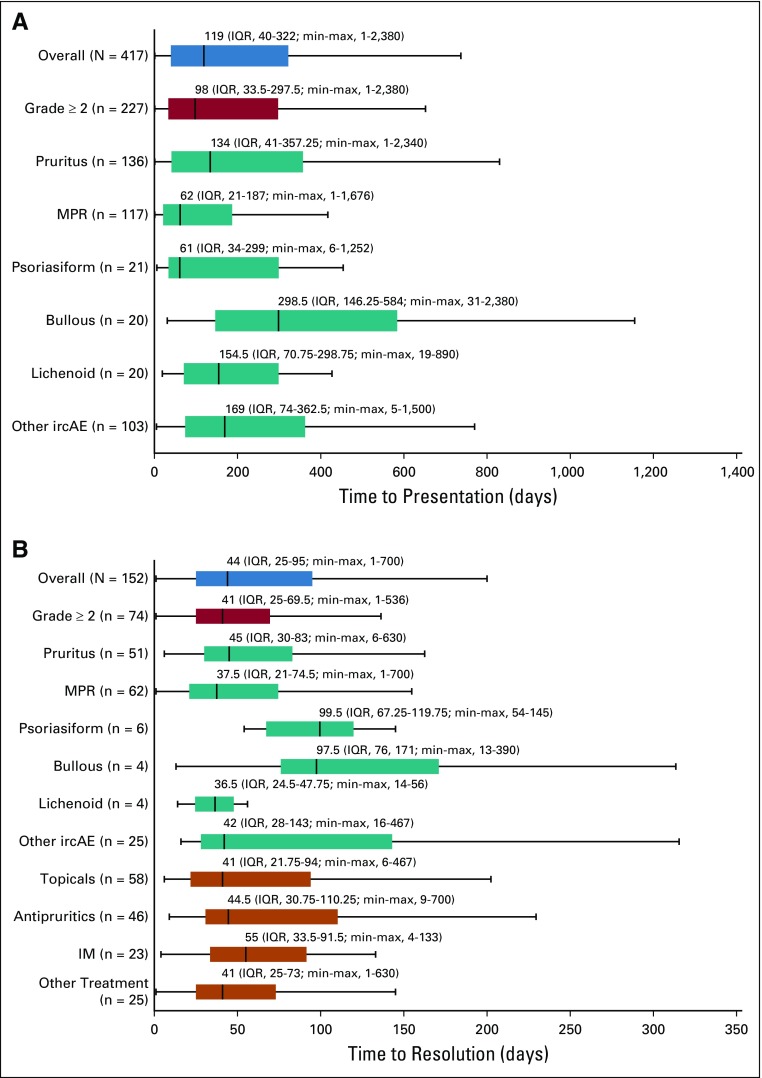
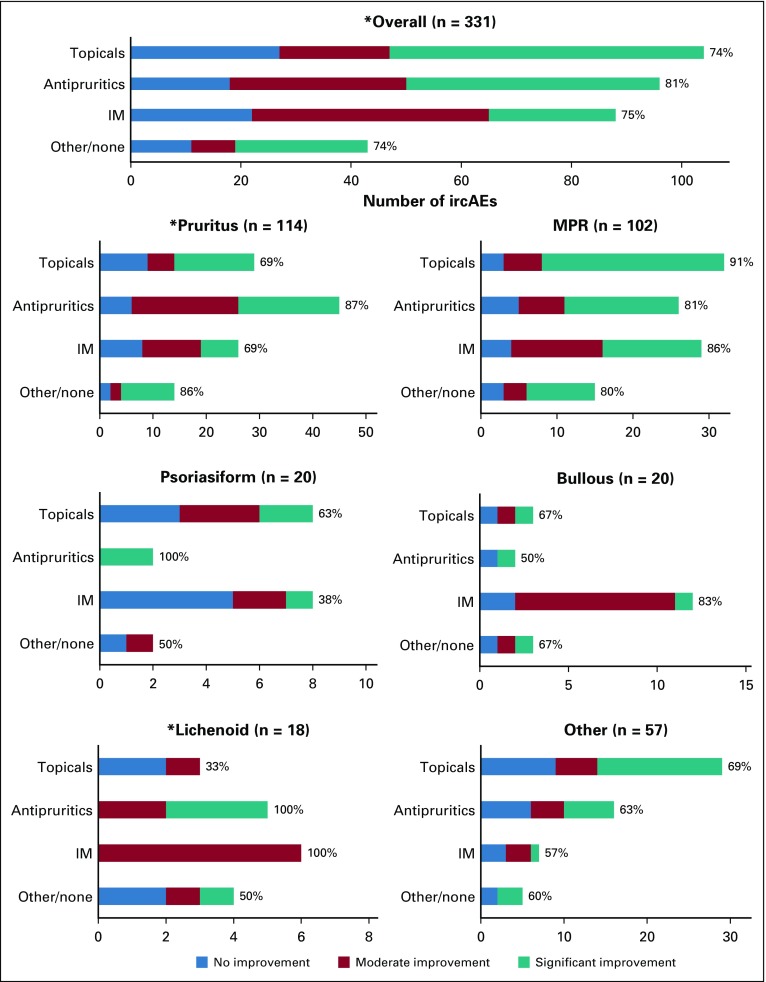
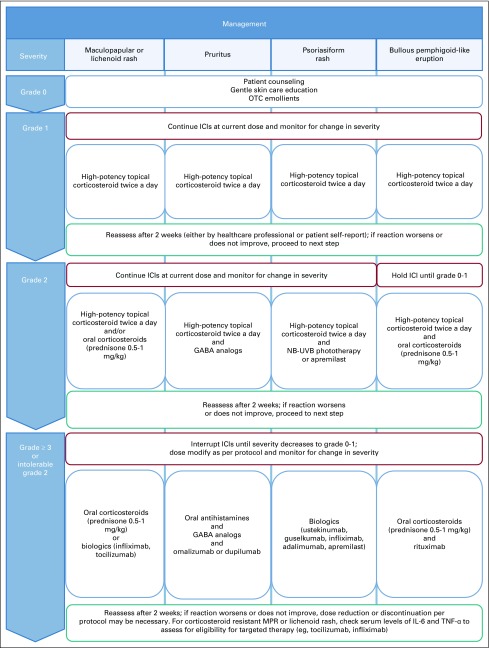
Results: A total of 285 patients (median age, 65 years [range, 17 to 89 years]) with 427 ircAEs were included: pruritus (n = 138; 32%), maculopapular rash (n = 120; 28%), psoriasiform rash (n = 22; 5%), and others (n = 147; 34%). Immune checkpoint inhibitor class was associated with ircAE phenotype (P = .007), where maculopapular rash was predominant in patients who received combination therapy. Severity of ircAEs was significantly reduced (mean Common Terminology Criteria for Adverse Events grade: 1.74 v 0.71; P < .001) with dermatologic interventions, including topical corticosteroids, oral antipruritics, and systemic immunomodulators. A total of 88 ircAEs (20%) were managed with systemic immunomodulators. Of these, 22 (25%) of 88 persisted or worsened. In seven patients with corticosteroid-refractory ircAEs, improvement resulted from targeted biologic immunomodulatory therapies that included rituximab and dupilumab. Serum interleukin-6 (IL-6) was elevated in 34 (52%) of 65 patients; grade 3 or greater ircAEs were associated with increased absolute eosinophils (odds ratio, 4.1; 95% CI, 1.3 to 13.4) and IL-10 (odds ratio, 23.8; 95% CI, 2.1 to 262.5); mean immunoglobulin E serum levels were greater in higher-grade ircAEs: 1,093 kU/L (grade 3), 245 kU/L (grade 2), and 112 kU/L (grade 1; P = .043).
Conclusion: Most ircAEs responded to symptom- and phenotype-directed dermatologic therapies, whereas biologic therapies were effective in patients with corticosteroid-refractory disease. Increased eosinophils, IL-6, IL-10, and immunoglobulin E were associated with ircAEs, and they may represent actionable therapeutic targets for immune-related skin toxicities.
Conflict of interest statement
The content is solely the responsibility of the authors and does not necessarily represent the official views of the US National Institutes of Health. The sponsors had no role in the design and conduct of the study; in the collection, analysis, and interpretation of data; in the preparation, review, or approval of the manuscript; or in the decision to submit the manuscript for publication.
Figures
References
-
- Malkhasyan KA, Zakharia Y, Milhem M. Quality-of-life outcomes in patients with advanced melanoma: A review of the literature. Pigment Cell Melanoma Res. 2017;30:511–520. - PubMed
-
- Brahmer JR, Rodríguez-Abreu D, Robinson AG, et al. Health-related quality-of-life results for pembrolizumab versus chemotherapy in advanced, PD-L1-positive NSCLC (KEYNOTE-024): A multicentre, international, randomised, open-label phase 3 trial. Lancet Oncol. 2017;18:1600–1609. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
