

Comparison of Conventional Lipoprotein Tests and Apolipoproteins in the Prediction of Cardiovascular Disease
- PMID: 31216866
- PMCID: PMC6693929
- DOI: 10.1161/CIRCULATIONAHA.119.041149
Comparison of Conventional Lipoprotein Tests and Apolipoproteins in the Prediction of Cardiovascular Disease
Abstract
Background: Total cholesterol and high-density lipoprotein cholesterol (HDL-C) measurements are central to cardiovascular disease (CVD) risk assessment, but there is continuing debate around the utility of other lipids for risk prediction.
Methods: Participants from UK Biobank without baseline CVD and not taking statins, with relevant lipid measurements (n=346 686), were included in the primary analysis. An incident fatal or nonfatal CVD event occurred in 6216 participants (1656 fatal) over a median of 8.9 years. Associations of nonfasting lipid measurements (total cholesterol, HDL-C, non-HDL-C, direct and calculated low-density lipoprotein cholesterol [LDL-C], and apolipoproteins [Apo] A1 and B) with CVD were compared using Cox models adjusting for classical risk factors, and predictive utility was determined by the C-index and net reclassification index. Prediction was also tested in 68 649 participants taking a statin with or without baseline CVD (3515 CVD events).
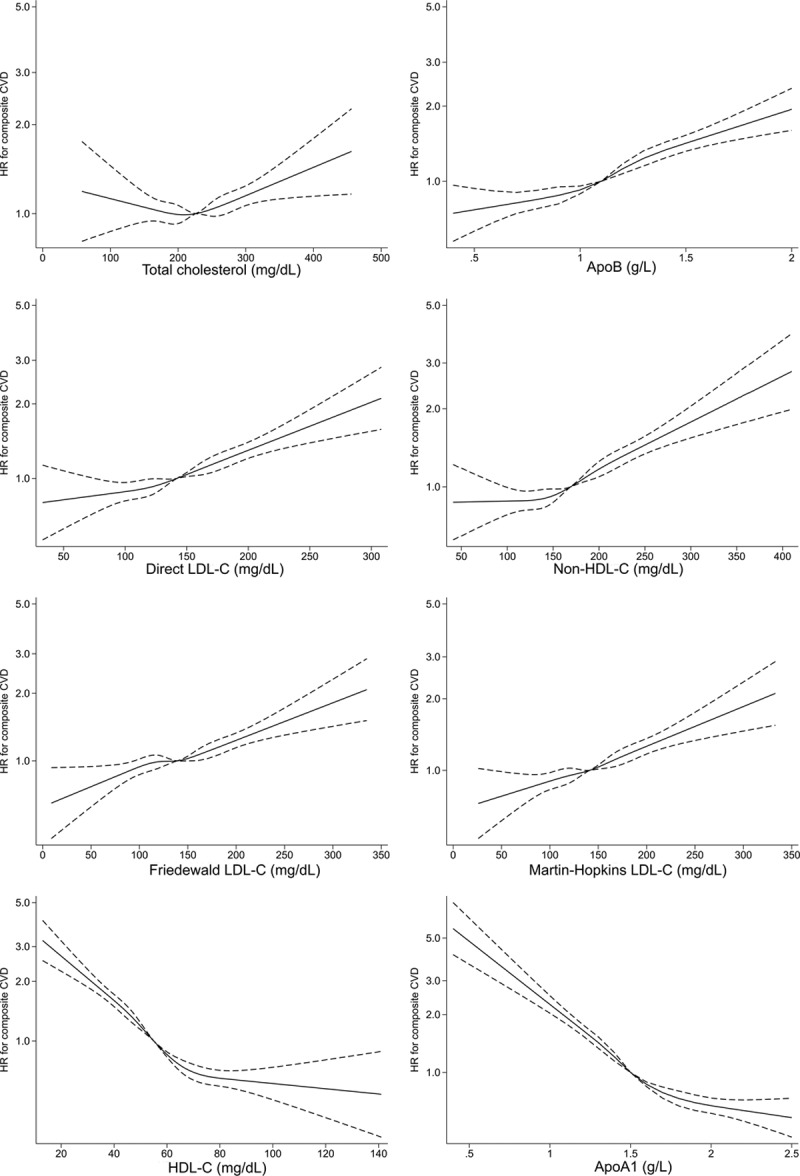
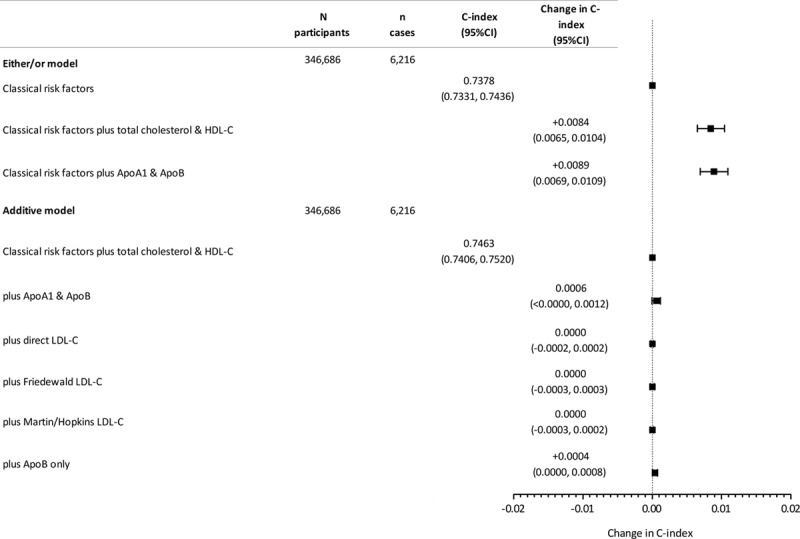
Results: ApoB, LDL-C, and non-HDL-C were highly correlated (r>0.90), while HDL-C was strongly correlated with ApoA1 (r=0.92). After adjustment for classical risk factors, 1 SD increase in ApoB, direct LDL-C, and non-HDL-C had similar associations with composite fatal/nonfatal CVD events (hazard ratio, 1.23, 1.20, 1.21, respectively). Associations for 1 SD increase in HDL-C and ApoA1 were also similar (hazard ratios, 0.81 [both]). Adding either total cholesterol and HDL-C, or ApoB and ApoA, to a CVD risk prediction model (C-index, 0.7378) yielded similar improvement in discrimination (C-index change, 0.0084; 95% CI, 0.0065, 0.0104, and 0.0089; 95% CI, 0.0069, 0.0109, respectively). Once total and HDL-C were in the model, no further substantive improvement was achieved with the addition of ApoB (C-index change, 0.0004; 95% CI, 0.0000, 0.0008) or any measure of LDL-C. Results for predictive utility were similar for a fatal CVD outcome, and in a discordance analysis. In participants taking a statin, classical risk factors (C-index, 0.7118) were improved by non-HDL-C (C-index change, 0.0030; 95% CI, 0.0012, 0.0048) or ApoB (C-index change, 0.0030; 95% CI, 0.0011, 0.0048). However, adding ApoB or LDL-C to a model already containing non-HDL-C did not further improve discrimination.
Conclusions: Measurement of total cholesterol and HDL-C in the nonfasted state is sufficient to capture the lipid-associated risk in CVD prediction, with no meaningful improvement from addition of apolipoproteins, direct or calculated LDL-C.
Keywords: apolipoprotein A-1; apolipoprotein B; cardiovascular diseases; cholesterol, HDL; cholesterol, LDL.
Figures
Comment in
-
Cholesterol Insights and Controversies From the UK Biobank Study.Circulation. 2019 Aug 13;140(7):553-555. doi: 10.1161/CIRCULATIONAHA.119.042134. Epub 2019 Aug 12. Circulation. 2019. PMID: 31403842 Free PMC article. No abstract available.
-
Letter by Sniderman et al Regarding Article, "Comparison of Conventional Lipoprotein Tests and Apolipoproteins in the Prediction of Cardiovascular Disease".Circulation. 2019 Dec 10;140(24):e822-e823. doi: 10.1161/CIRCULATIONAHA.119.042776. Epub 2019 Dec 9. Circulation. 2019. PMID: 31815544 No abstract available.
-
Response by Welsh et al to Letter Regarding Article, "Comparison of Conventional Lipoprotein Tests and Apolipoproteins in the Prediction of Cardiovascular Disease".Circulation. 2019 Dec 10;140(24):e824-e825. doi: 10.1161/CIRCULATIONAHA.119.044325. Epub 2019 Dec 9. Circulation. 2019. PMID: 31815545 No abstract available.
References
-
- Arsenault BJ, Boekholdt SM, Kastelein JJ. Lipid parameters for measuring risk of cardiovascular disease. Nat Rev Cardiol. 2011;8:197–206. doi: 10.1038/nrcardio.2010.223. - PubMed
-
- Mihaylova B, Emberson J, Blackwell L, Keech A, Simes J, Barnes EH, Voysey M, Gray A, Collins R, Baigent C, et al. The effects of lowering LDL cholesterol with statin therapy in people at low risk of vascular disease: meta-analysis of individual data from 27 randomised trials. Lancet. 2012;380:581–590. - PMC - PubMed
-
- Sabatine MS, Giugliano RP, Keech AC, Honarpour N, Wiviott SD, Murphy SA, Kuder JF, Wang H, Liu T, Wasserman SM, et al. FOURIER Steering Committee and Investigators. Evolocumab and clinical outcomes in patients with cardiovascular disease. N Engl J Med. 2017;376:1713–1722. doi: 10.1056/NEJMoa1615664. - PubMed
-
- Piepoli MF, Hoes AW, Agewall S, Albus C, Brotons C, Catapano AL, Cooney M-T, Corrà U, Cosyns B, Deaton C, et al. 2016 European Guidelines on cardiovascular disease prevention in clinical practice. Atherosclerosis. 2016;252:207–274. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
