

Prevalence, Risk Factors, and Outcomes of Bacteremic Pneumonia in Children
- PMID: 31217309
- PMCID: PMC6615516
- DOI: 10.1542/peds.2018-3090
Prevalence, Risk Factors, and Outcomes of Bacteremic Pneumonia in Children
Abstract
Background: Previous studies examining bacteremia in hospitalized children with pneumonia are limited by incomplete culture data. We sought to determine characteristics of children with bacteremic pneumonia using data from a large prospective study with systematic blood culturing.
Methods: Children <18 years hospitalized with pneumonia and enrolled in the multicenter Etiology of Pneumonia in the Community study between January 2010 and June 2012 were eligible. Bivariate comparisons were used to identify factors associated with bacteremia. Associations between bacteremia and clinical outcomes were assessed by using Cox proportional hazards regression for length of stay and logistic regression for ICU admission and invasive mechanical ventilation or shock.
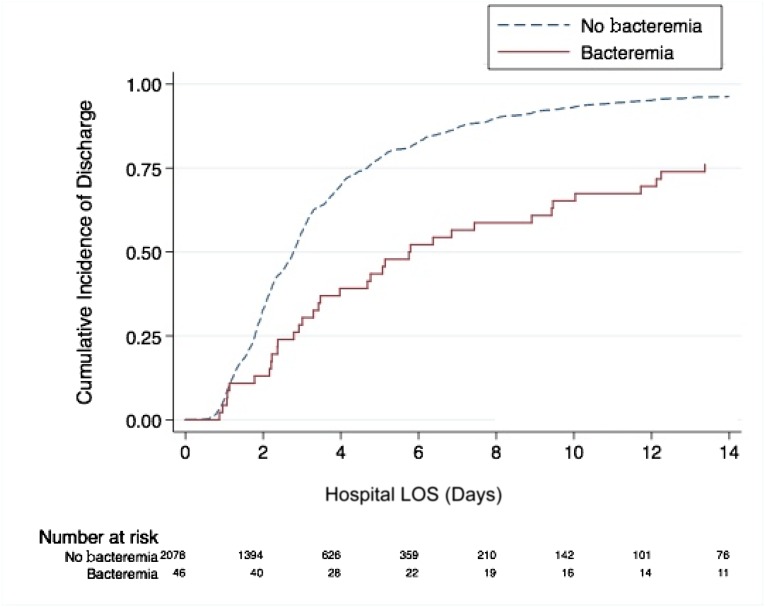
Results: Blood cultures were obtained in 2143 (91%) of 2358 children; 46 (2.2%) had bacteremia. The most common pathogens were Streptococcus pneumoniae (n = 23, 50%), Staphylococcus aureus (n = 6, 13%), and Streptococcus pyogenes (n = 4, 9%). Characteristics associated with bacteremia included male sex, parapneumonic effusion, lack of chest indrawing or wheezing, and no previous receipt of antibiotics. Children with bacteremia had longer lengths of stay (median: 5.8 vs 2.8 days; adjusted hazard ratio: 0.79 [0.73-0.86]) and increased odds of ICU admission (43% vs 21%; adjusted odds ratio: 5.21 [3.82-6.84]) and invasive mechanical ventilation or shock (30% vs 8%; adjusted odds ratio: 5.28 [2.41-11.57]).
Conclusions: Bacteremia was uncommonly detected in this large multicenter cohort of children hospitalized with community-acquired pneumonia but was associated with severe disease. S pneumoniae was detected most often. Blood culture was of low yield in general but may have greater use in those with parapneumonic effusion and ICU admission.
Copyright © 2019 by the American Academy of Pediatrics.
Conflict of interest statement
POTENTIAL CONFLICT OF INTEREST: Dr Ampofo has received consulting fees from Merck. Dr Anderson has received grant support through his institution from MedImmune, Pfizer, Merck, Sanofi Pasteur, PaxVax, Novavax, and Micron Biomedical and consulting fees from AbbVie. Dr Grijalva has received consulting fees from Pfizer, Sanofi, and Merck and received research support from Sanofi Pasteur, Campbell Alliance, the Centers for Disease Control and Prevention, National Institutes of Health, Food and Drug Administration, and Agency for Health Care Research and Quality. Dr Pavia has received consulting fees from Genentech. The other authors have indicated they have no potential conflicts of interest to disclose.
Figures
Similar articles
-
Bacteremia in Staphylococcus aureus pneumonia: outcomes and epidemiology.J Crit Care. 2011 Aug;26(4):395-401. doi: 10.1016/j.jcrc.2010.09.002. Epub 2010 Oct 30. J Crit Care. 2011. PMID: 21036521
-
Utility of Blood Culture Among Children Hospitalized With Community-Acquired Pneumonia.Pediatrics. 2017 Sep;140(3):e20171013. doi: 10.1542/peds.2017-1013. Epub 2017 Aug 23. Pediatrics. 2017. PMID: 28835382 Free PMC article.
-
[Clinical predictors of bacteremia in immunocompetent adult patients hospitalized for community-acquired pneumonia].Rev Med Chil. 2015 May;143(5):553-61. doi: 10.4067/S0034-98872015000500001. Rev Med Chil. 2015. PMID: 26203565 Spanish.
-
Optimizing treatment outcomes in severe community-acquired pneumonia.Am J Respir Med. 2003;2(1):39-54. doi: 10.1007/BF03256638. Am J Respir Med. 2003. PMID: 14720021 Review.
-
Severe community-acquired pneumonia.Infect Dis Clin North Am. 2009 Sep;23(3):503-20. doi: 10.1016/j.idc.2009.04.003. Infect Dis Clin North Am. 2009. PMID: 19665080 Review.
Cited by
-
Profile of Bacteria with ARGs Among Real-World Samples from ICU Admission Patients with Pulmonary Infection Revealed by Metagenomic NGS.Infect Drug Resist. 2021 Nov 27;14:4993-5004. doi: 10.2147/IDR.S335864. eCollection 2021. Infect Drug Resist. 2021. PMID: 34866919 Free PMC article.
-
Challenges of Antibiotic Stewardship in the Pediatric and Neonatal Intensive Care Units.J Pediatr Pharmacol Ther. 2021;26(7):659-668. doi: 10.5863/1551-6776-26.7.659. Epub 2021 Sep 24. J Pediatr Pharmacol Ther. 2021. PMID: 34588929 Free PMC article.
-
Adenovirus and Mycoplasma pneumoniae co-infection as a risk factor for severe community-acquired pneumonia in children.Front Pediatr. 2024 Jan 31;12:1337786. doi: 10.3389/fped.2024.1337786. eCollection 2024. Front Pediatr. 2024. PMID: 38357505 Free PMC article.
-
Anti-PD-L1 Therapy Does Not Improve Survival in a Murine Model of Lethal Staphylococcus aureus Pneumonia.J Infect Dis. 2021 Dec 15;224(12):2073-2084. doi: 10.1093/infdis/jiab274. J Infect Dis. 2021. PMID: 34009385 Free PMC article.
-
Sex and Gender Differences in Bacterial Infections.Infect Immun. 2022 Oct 20;90(10):e0028322. doi: 10.1128/iai.00283-22. Epub 2022 Sep 19. Infect Immun. 2022. PMID: 36121220 Free PMC article. Review.
References
-
- Witt W, Weiss A, Elixhauser A. Overview of Hospital Stays for Children in the United States, 2012. Statistical Brief #187. Rockville, MD: Agency for Healthcare Research and Quality; 2014 - PubMed
-
- Bradley JS, Byington CL, Shah SS, et al. ; Pediatric Infectious Diseases Society and the Infectious Diseases Society of America . Executive summary: the management of community-acquired pneumonia in infants and children older than 3 months of age: clinical practice guidelines by the Pediatric Infectious Diseases Society and the Infectious Diseases Society of America. Clin Infect Dis. 2011;53(7):617–630 - PMC - PubMed
-
- Iroh Tam PY, Bernstein E, Ma X, Ferrieri P. Blood culture in evaluation of pediatric community-acquired pneumonia: a systematic review and meta-analysis. Hosp Pediatr. 2015;5(6):324–336 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
