

Sigmoido-rectal intussusception
- PMID: 31217975
- PMCID: PMC6558527
- DOI: 10.1177/2050313X19856242
Sigmoido-rectal intussusception
Abstract
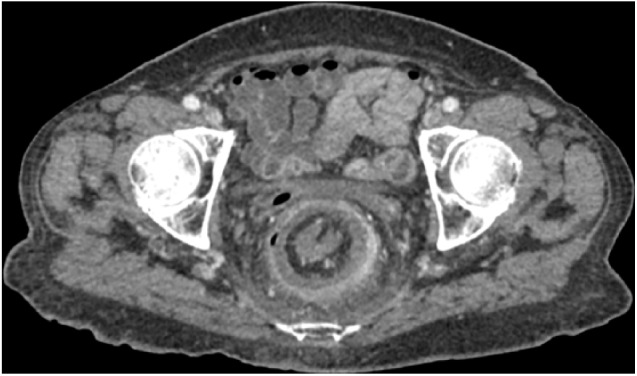
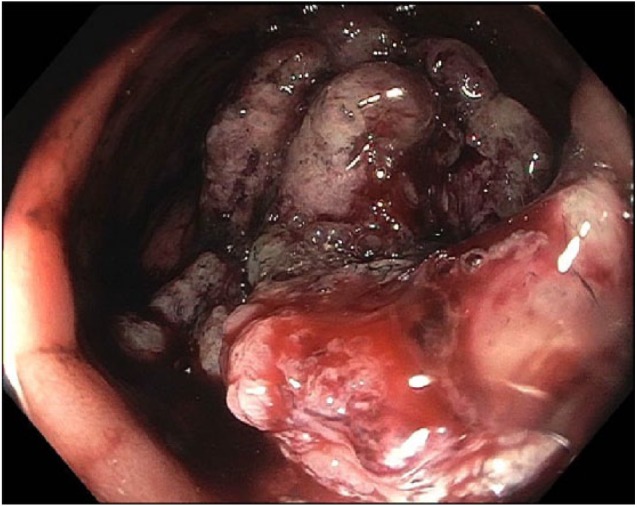
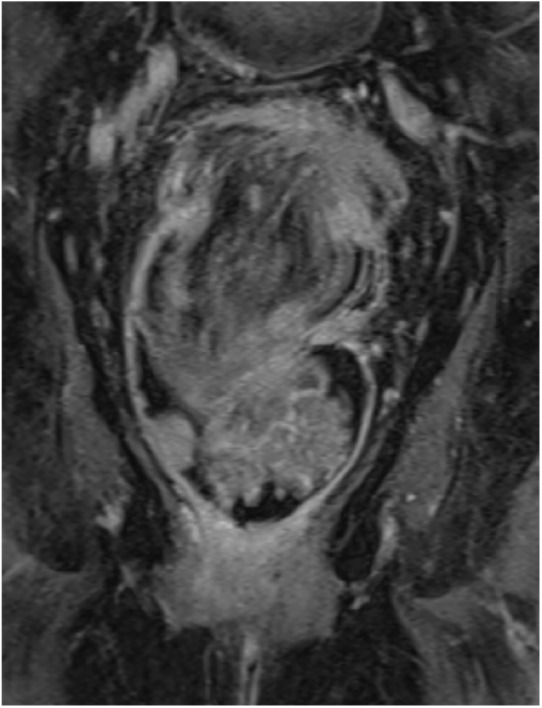
Rectal prolapse is usually of benign etiology. Rarely, sigmoido-rectal intussusception results from a malignant lead-point. We report the case of a patient with a partially obstructing sigmoid cancer causing a full thickness rectal prolapse requiring surgical intervention. An 82-year-old woman presented with 1 week of rectal bleeding, fecal incontinence, and weight loss. Computed tomography identified sigmoido-rectal intussusception. Colonoscopic biopsy revealed high-grade dysplasia. Magnetic resonance imaging demonstrated a 6-cm mass forming the lead point of the intussusceptum with epiploic appendages seen within the rectal lumen. She underwent laparoscopic low anterior resection with final pathology consistent with T2N0 adenocarcinoma, and recovered well. Among adult patients with rectal prolapse, suspicion for underlying malignancy should prompt a thorough investigation to inform the decision for resection, which may be safely performed by minimally invasive techniques.
Keywords: cancer; computed tomography; gastroenterology/hepatology; imaging; intussusception; magnetic resonance imaging; oncology; rectal prolapse; surgery.
Conflict of interest statement
Declaration of conflicting interests: The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Figures
References
-
- Takeuchi K, Tsuzuki Y, Ando T, et al. The diagnosis and treatment of adult intussusception. J Clin Gastroenterol 2003; 36(1): 18–21. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
