

Outcomes of cardiac resynchronisation therapy in patients with heart failure with atrial fibrillation: a systematic review and meta-analysis of observational studies
- PMID: 31217991
- PMCID: PMC6546263
- DOI: 10.1136/openhrt-2018-000937
Outcomes of cardiac resynchronisation therapy in patients with heart failure with atrial fibrillation: a systematic review and meta-analysis of observational studies
Abstract
Background: Cardiac resynchronisation therapy (CRT) is beneficial in selected patients with heart failure (HF) in normal sinus rhythm (NSR). We sought to evaluate the impact of CRT with or without atrioventricular junction (AVJ) ablation in patients with HF with concomitant atrial fibrillation (AF).
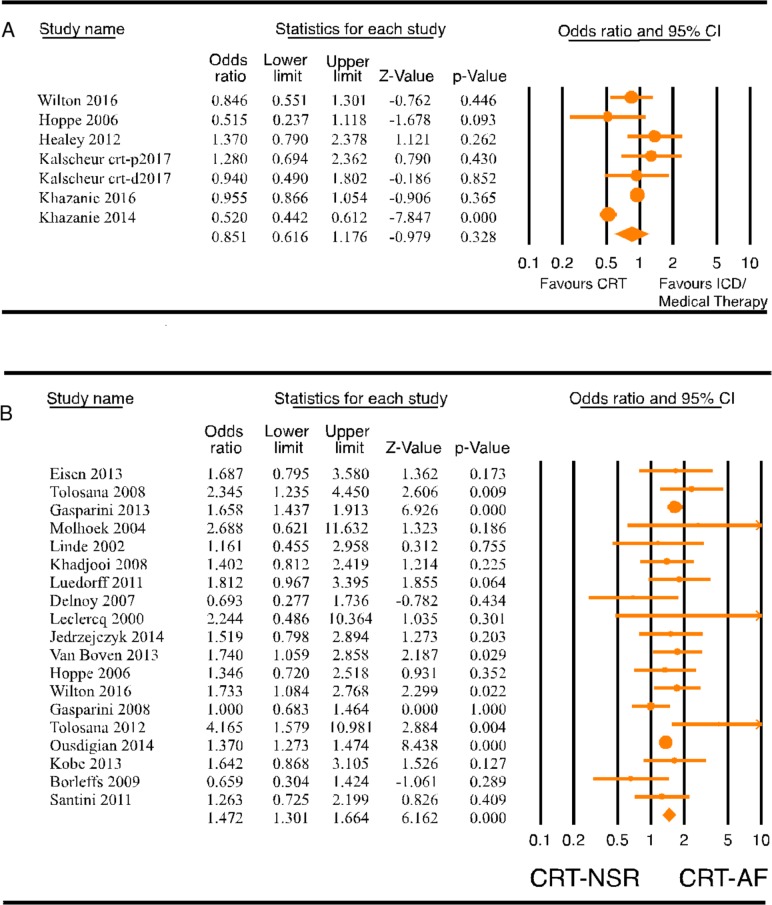
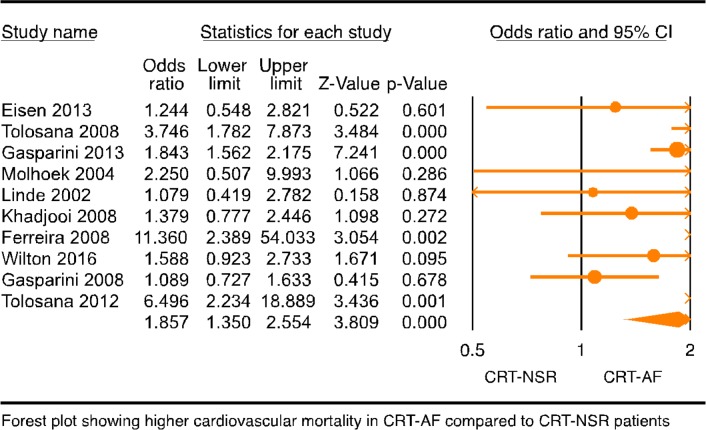
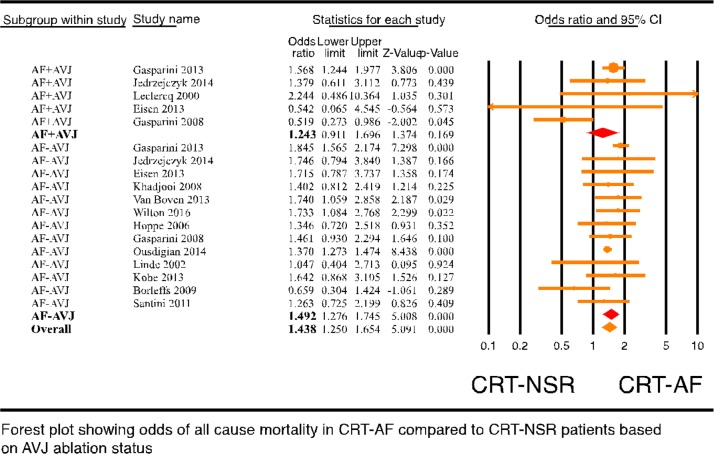
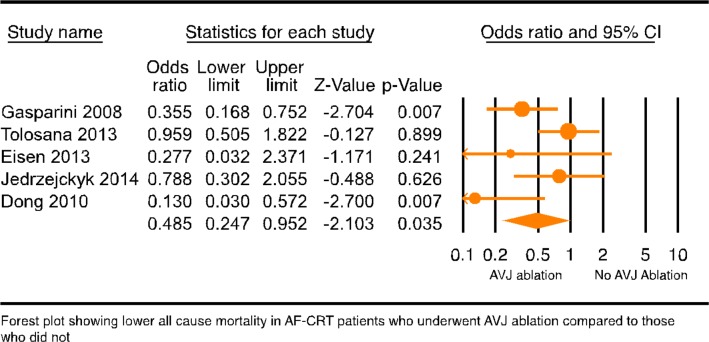
Methods and results: Literature was searched (inception through 30 August 2017) for observational studies that reported outcomes in patients with HF with CRT and AF that reported all-cause and cardiovascular mortality. Thirty-one studies with 83, 571 patients were included. CRT did not decrease mortality compared with internal cardioverter defibrillator or medical therapy alone in patients with HF and AF with indications for CRT (OR: 0.851, 95% CI 0.616 to 1.176, p=0.328, I2=86.954). CRT-AF patients had significantly higher all-cause and cardiovascular mortality than CRT-NSR patients ([OR: 1.472, 95% CI 1.301 to 1.664, p=0.000] and [OR: 1.857, 95% CI 1.350 to 2.554, p=0.000] respectively). Change in left ventricular ejection fraction was not different between CRT patients with and without AF (p=0.705). AVJ ablation, however, improved all-cause mortality in CRT-AF patients when compared with CRT-AF patients without AVJ ablation (OR: 0.485, 95% CI 0.247 to 0.952, p=0.035). With AVJ ablation, there was no difference in all-cause mortality in CRT-AF patients compared with CRT-NSR patients (OR: 1.245, 95% CI 0.914 to 1.696, p=0.165).
Conclusion: The results of our meta-analysis suggest that AF was associated with decreased CRT benefits in patients with HF. CRT, however, benefits patients with AF with AVJ ablation.
Keywords: atrioventricular junction ablation; biventricular pacing; ejection fraction; implanted cardioverter defibrillator.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- Tolosana JM, Hernandez Madrid A, Brugada J, et al. . Comparison of benefits and mortality in cardiac resynchronization therapy in patients with atrial fibrillation versus patients in sinus rhythm (Results of the Spanish Atrial Fibrillation and Resynchronization [SPARE] Study). Am J Cardiol 2008;102:444–9. 10.1016/j.amjcard.2008.04.008 - DOI - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous