

Current status of surgery first approach (part II): precautions and complications
- PMID: 31218215
- PMCID: PMC6546776
- DOI: 10.1186/s40902-019-0206-4
Current status of surgery first approach (part II): precautions and complications
Abstract
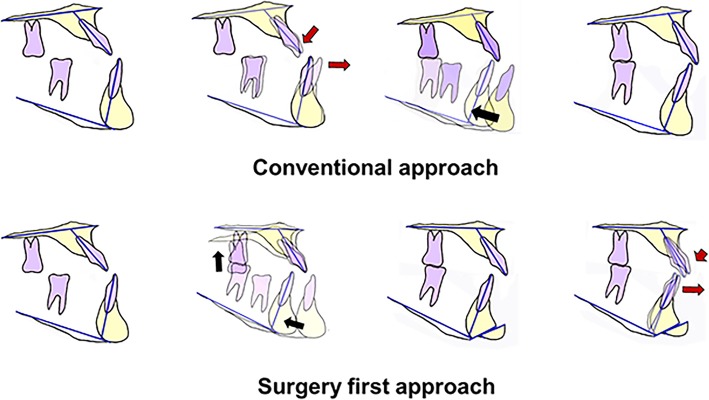
The choice of surgical technique in orthognathic surgery is based primarily on the surgical treatment objectives (STO), which is a fundamental component of the orthognathic treatment process. In the conventional orthodontics-first approach, presurgical planning can be performed twice, during the preorthodontic (initial STO) and presurgical phases (final STO). Recently, a surgery-first orthognathic approach (SFA) without presurgical orthodontic treatment has been introduced and combined initial and final STO at the same time. In contrast to the conventional surgical-orthodontic treatment protocol that includes preoperative orthodontics for dental decompensations to maximize stable postoperative occlusion, the SFA potentially shortens the treatment period and minimizes esthetic concerns during the decompensation period because skeletal problems are corrected from the beginning. The indications for the SFA have been proposed in the literature, but no consensus exists. Moreover, because dental occlusion of the pre-orthodontic arches cannot be used as a guide for establishing the surgical treatment plan, there are fundamental limitations in accurate prediction of postsurgical results in the SFA. Recently, the concepts of postsurgical orthodontic treatment are continuously changing and evolving to overcome this inherent limitation of the SFA. The elimination of presurgical orthodontics can change the paradigm of orthognathic surgery but still requires cautious case selection and thorough discussion and collaboration between orthodontists and surgeons regarding the goals and postoperative management of the orthognathic procedure.
Keywords: Complications; Orthodontics; Orthognathic surgery; Stability; Surgery first.
Conflict of interest statement
Competing interestsThe authors declare that they have no competing interests.
Figures




Similar articles
-
An overview of surgery-first orthognathic approach: History, indications and limitations, protocols, and dentoskeletal stability.Dent Res J (Isfahan). 2021 Jun 22;18:47. eCollection 2021. Dent Res J (Isfahan). 2021. PMID: 34429867 Free PMC article. Review.
-
Rationale, Relevance, and Efficacy of "Surgery First, Orthodontics Later" Approach in the Management of Cases of Severe Malocclusion with Skeletal Discrepancy.Ann Maxillofac Surg. 2019 Jan-Jun;9(1):57-71. doi: 10.4103/ams.ams_272_18. Ann Maxillofac Surg. 2019. PMID: 31293931 Free PMC article.
-
Large-Scale Study of Long-Term Vertical Skeletal Stability in a Surgery-First Orthognathic Approach Without Presurgical Orthodontic Treatment: Part II.J Craniofac Surg. 2018 Jun;29(4):953-958. doi: 10.1097/SCS.0000000000004433. J Craniofac Surg. 2018. PMID: 29521747
-
The reliability of a surgery-first orthognathic approach without presurgical orthodontic treatment for skeletal class III dentofacial deformity.Ann Plast Surg. 2015 Mar;74(3):333-41. doi: 10.1097/SAP.0b013e318295dcce. Ann Plast Surg. 2015. PMID: 23838836 Clinical Trial.
-
Surgery-First Approach; from Claims to Evidence: A Comprehensive Review.Front Dent. 2022 Aug 3;19:23. doi: 10.18502/fid.v19i23.10594. eCollection 2022. Front Dent. 2022. PMID: 36458270 Free PMC article. Review.
Cited by
-
Current Orthognathic Practice in India: Do We Need to Change?J Maxillofac Oral Surg. 2020 Mar;19(1):1-11. doi: 10.1007/s12663-019-01269-y. Epub 2019 Aug 17. J Maxillofac Oral Surg. 2020. PMID: 31988555 Free PMC article. Review.
-
Effect of surgery-first approach on quality of life and mental health of orthognathic patients: A systematic review and meta-analysis.Heliyon. 2023 Dec 3;10(1):e23285. doi: 10.1016/j.heliyon.2023.e23285. eCollection 2024 Jan 15. Heliyon. 2023. PMID: 38163099 Free PMC article.
-
An overview of surgery-first orthognathic approach: History, indications and limitations, protocols, and dentoskeletal stability.Dent Res J (Isfahan). 2021 Jun 22;18:47. eCollection 2021. Dent Res J (Isfahan). 2021. PMID: 34429867 Free PMC article. Review.
-
The effect of 4-hexylresorinol administration on NAD+ level and SIRT activity in Saos-2 cells.Maxillofac Plast Reconstr Surg. 2021 Nov 1;43(1):39. doi: 10.1186/s40902-021-00326-2. Maxillofac Plast Reconstr Surg. 2021. PMID: 34719767 Free PMC article.
-
Modern Surgery-First Approach Concept in Cleft-Orthognathic Surgery: A Comparative Cohort Study with 3D Quantitative Analysis of Surgical-Occlusion Setup.J Clin Med. 2019 Dec 2;8(12):2116. doi: 10.3390/jcm8122116. J Clin Med. 2019. PMID: 31810279 Free PMC article.
References
-
- Nagasaka H, Sugawara J, Kawamura H, Nanda R. “Surgery first” skeletal Class III correction using the Skeletal Anchorage System. J Clin Orthod. 2009;43:97–105. - PubMed
-
- Pelo S, Gasparini G, Garagiola U, Cordaro M, Di Nardo F, Staderini E, et al. Surgery-first orthognathic approach vs traditional orthognathic approach: oral health-related quality of life assessed with 2 questionnaires. Am J Orthod Dentofac Orthop. 2017;152:250–254. doi: 10.1016/j.ajodo.2016.12.022. - DOI - PubMed
-
- Park JK, Choi JY, Yang IH, Baek SH. Patient’s satisfaction in skeletal class III cases treated with two-jaw surgery using orthognathic quality of life questionnaire: conventional three-stage method versus surgery-first approach. J Craniofac Surg. 2015;26:2086–2093. doi: 10.1097/SCS.0000000000001972. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources