

Medical therapy doses at hospital discharge in patients with existing and de novo heart failure
- PMID: 31218850
- PMCID: PMC6676447
- DOI: 10.1002/ehf2.12454
Medical therapy doses at hospital discharge in patients with existing and de novo heart failure
Abstract
Aims: Uptitrating angiotensin-converting enzyme inhibitors or angiotensin receptor blockers (ACE-I/ARBs), beta-blockers, and mineralocorticoid receptor antagonists (MRAs) to optimal doses in heart failure with reduced ejection fraction (HFrEF) is associated with improved outcomes and recommended in guidelines. Studies of ambulatory patients found that a minority are prescribed optimal doses. However, dose at hospital discharge has rarely been reported. This information may guide quality improvement initiatives during and following discharge.
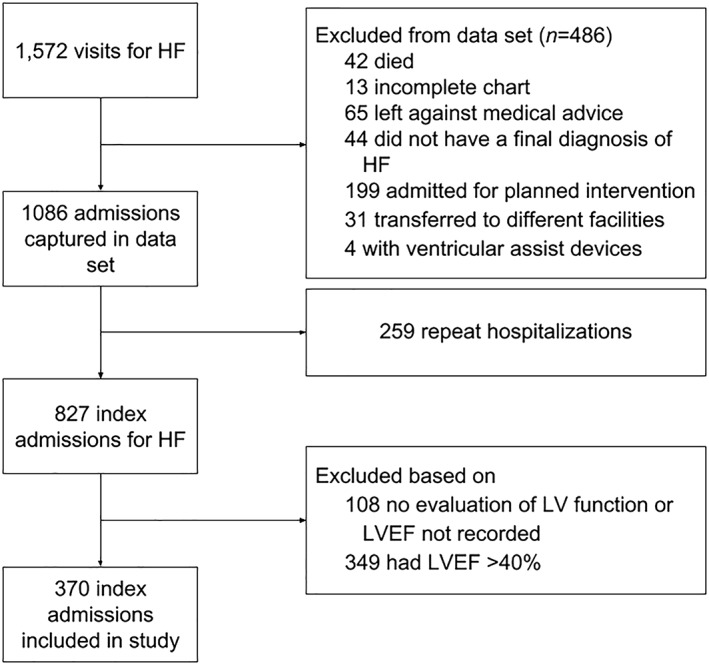
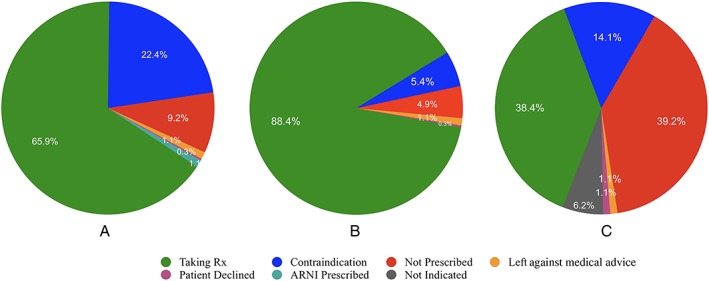
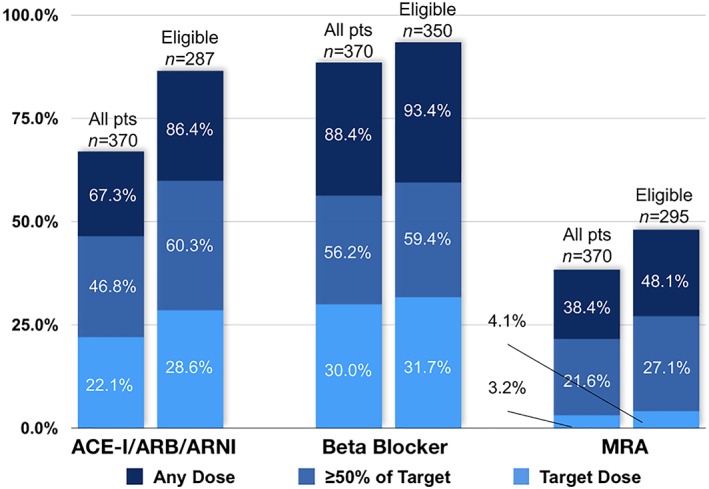
Methods and results: We assessed 370 consecutive patients with HFrEF hospitalized at two centres in Vancouver, Canada. Of those without contraindications, 86.4%, 93.4%, and 44.7% were prescribed an ACE-I/ARB/sacubitril-valsartan, beta-blocker, or MRA, respectively. The proportion of eligible patients prescribed target dose was respectively 28.6%, 31.7%, and 4.1%. Forty-two of 248 eligible patients (16.9%) were prescribed ≥50% of target dose, and only three patients received target dosing of all three medication classes. In multivariate regression models, cardiologist involvement in care was independently associated with increased dose and prescription of ≥50% of target dose for all medications, whereas a history of HF was only predictive for beta-blockers.
Conclusions: In a single-region experience of hospitalized HFrEF patients, a high proportion of eligible patients were discharged on ACE-I/ARB or beta-blocker. Less than half were prescribed MRAs, and few were prescribed ≥50% or target dosing of all medications. Further exploration into barriers to medication uptitration, and improvement in processes of care, is needed.
Keywords: Acute heart failure; Guideline adherence; Guideline-directed medical therapy; HFrEF; Systolic heart failure.
© 2019 The Authors. ESC Heart Failure published by John Wiley & Sons Ltd on behalf of the European Society of Cardiology.
Conflict of interest statement
None declared.
Figures
References
-
- WRITING COMMITTEE MEMBERS , Yancy CW, Jessup M, Bozkurt B, Butler J, Casey DE, Drazner MH, Fonarow GC, Geraci SA, Horwich T, Januzzi JL, Johnson MR, Kasper EK, Levy WC, Masoudi FA, McBride PE, McMurray JJV, Mitchell JE, Peterson PN, Riegel B, Sam F, Stevenson LW, Tang WHW, Tsai EJ, Wilkoff BL. 2013 ACCF/AHA guideline for the management of heart failure: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation 2013; 128: e240–e327. - PubMed
-
- Ponikowski P, Voors AA, Anker SD, Bueno H, Cleland JGF, Coats AJS, Falk V, González‐Juanatey JR, Harjola V‐P, Jankowska EA, Jessup M, Linde C, Nihoyannopoulos P, Parissis JT, Pieske B, Riley JP, Rosano GMC, Ruilope LM, Ruschitzka F, Rutten FH, van der Meer P. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur Heart J 2016; 37: 2129–2200. - PubMed
-
- Ezekowitz JA, O'Meara E, McDonald MA, Abrams H, Chan M, Ducharme A, Giannetti N, Grzeslo A, Hamilton PG, Heckman GA, Howlett JG, Koshman SL, Lepage S, McKelvie RS, Moe GW, Rajda M, Swiggum E, Virani SA, Zieroth S, Al‐Hesayen A, Cohen‐Solal A, D'Astous M, De S, Estrella‐Holder E, Fremes S, Green L, Haddad H, Harkness K, Hernandez AF, Kouz S, LeBlanc MH, Masoudi FA, Ross HJ, Roussin A, Sussex B. 2017 Comprehensive update of the Canadian Cardiovascular Society guidelines for the management of heart failure. Can J Cardiol 2017; 33: 1342–1433. - PubMed
-
- Jain A, Mills P, Nunn LM, Butler J, Luddington L, Ross V, Cliffe P, Ranjadayalan K, Timmis AD. Success of a multidisciplinary heart failure clinic for initiation and up‐titration of key therapeutic agents. Eur J Heart Fail 2005; 7: 405–410. - PubMed
-
- Calvert MJ, Shankar A, McManus RJ, Ryan R, Freemantle N. Evaluation of the management of heart failure in primary care. Fam Pract 2009; 26: 145–153. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
