

Pervasive wearable device for free tissue transfer monitoring based on advanced data analysis: clinical study report
- PMID: 31218875
- PMCID: PMC6977400
- DOI: 10.1117/1.JBO.24.6.067001
Pervasive wearable device for free tissue transfer monitoring based on advanced data analysis: clinical study report
Abstract
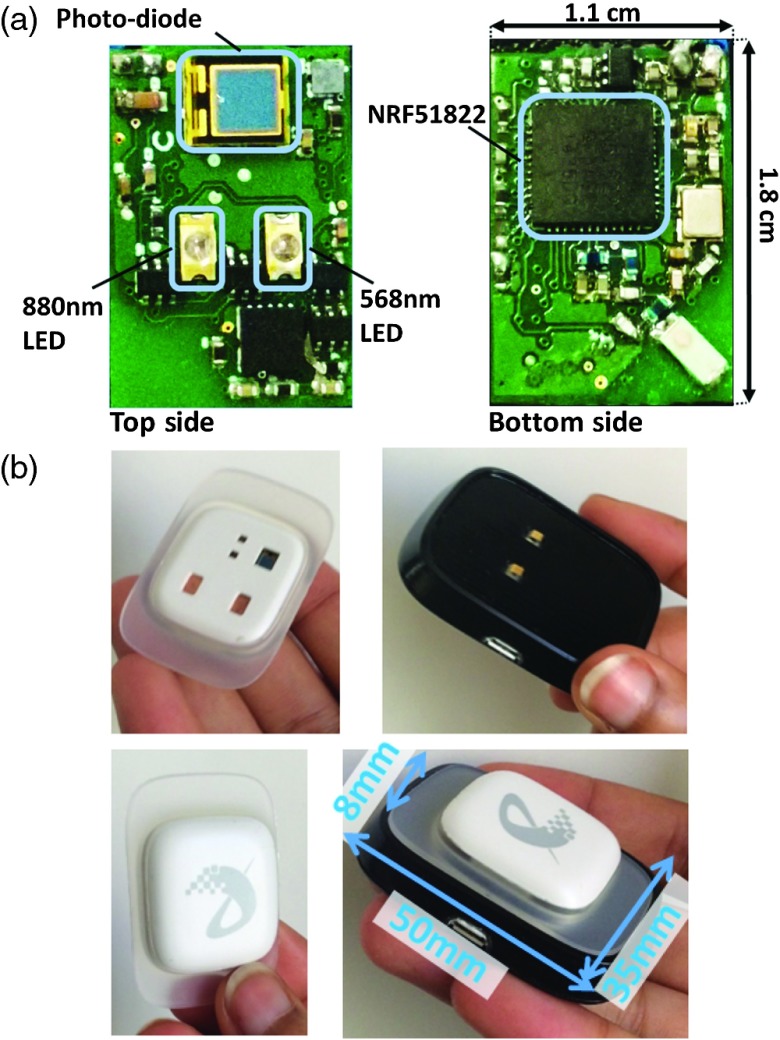
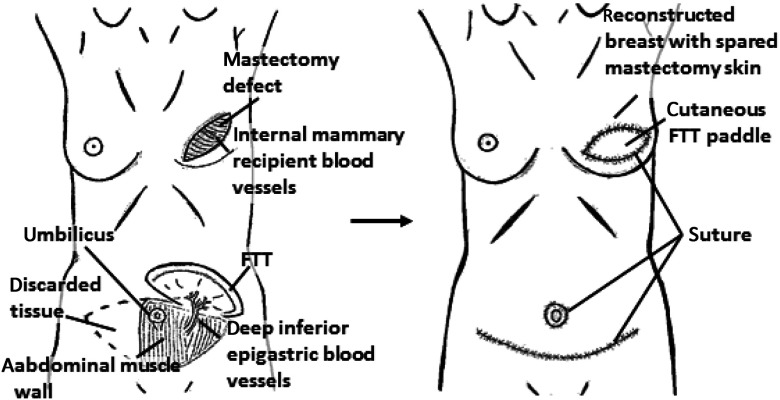
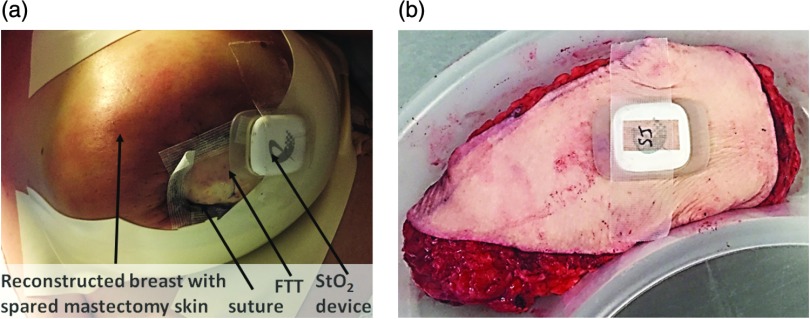
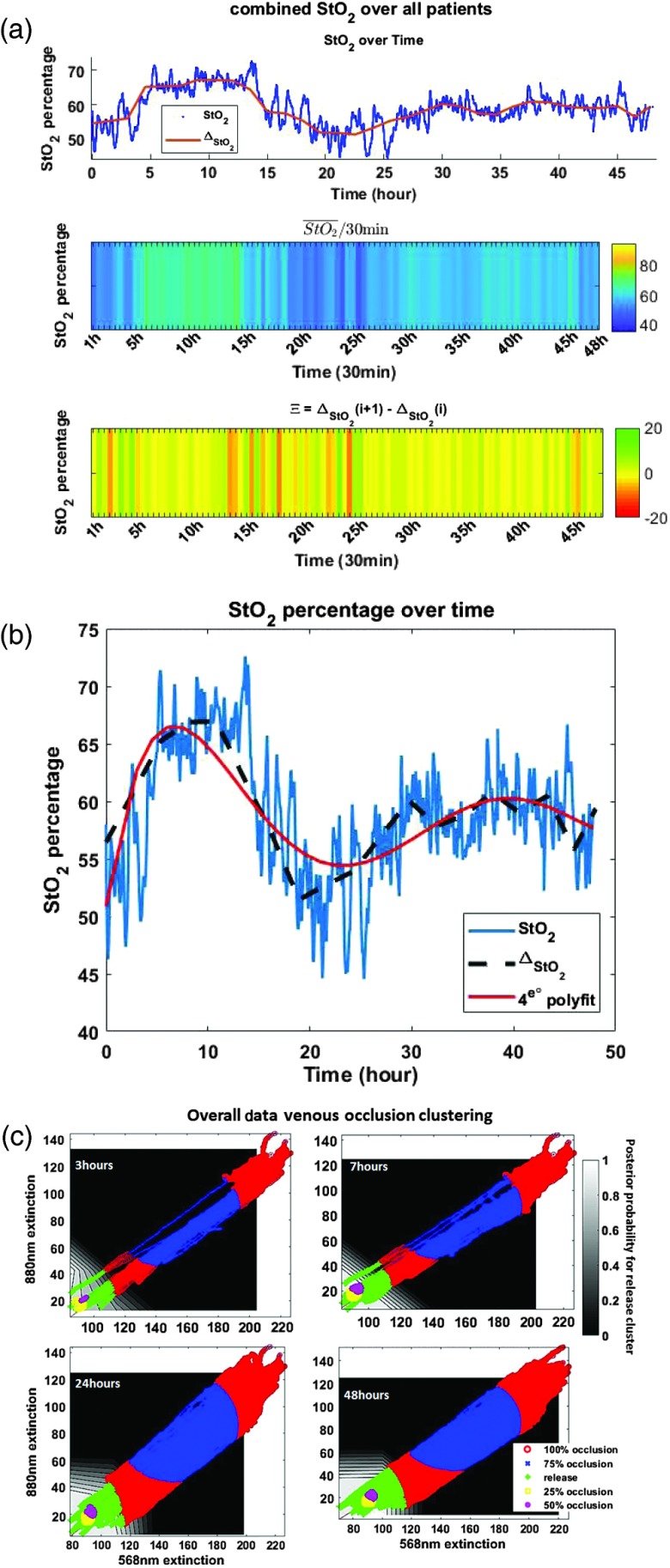
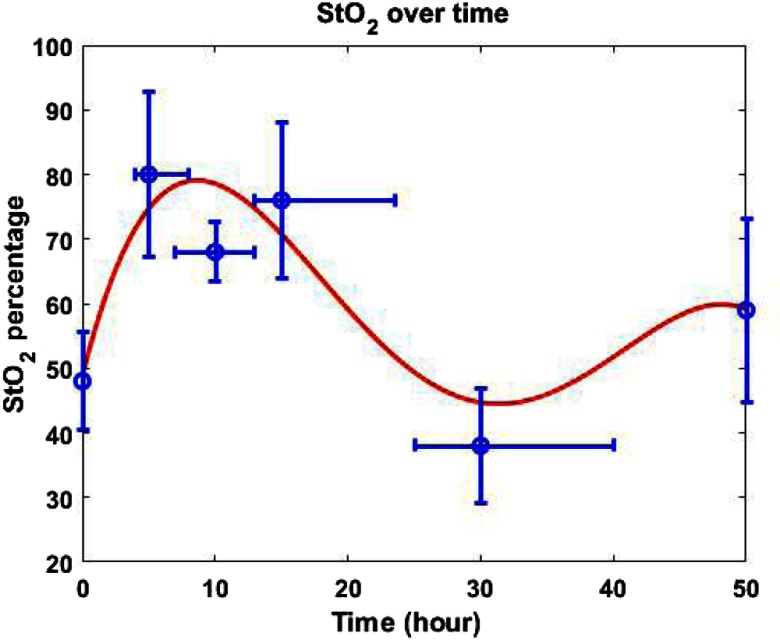
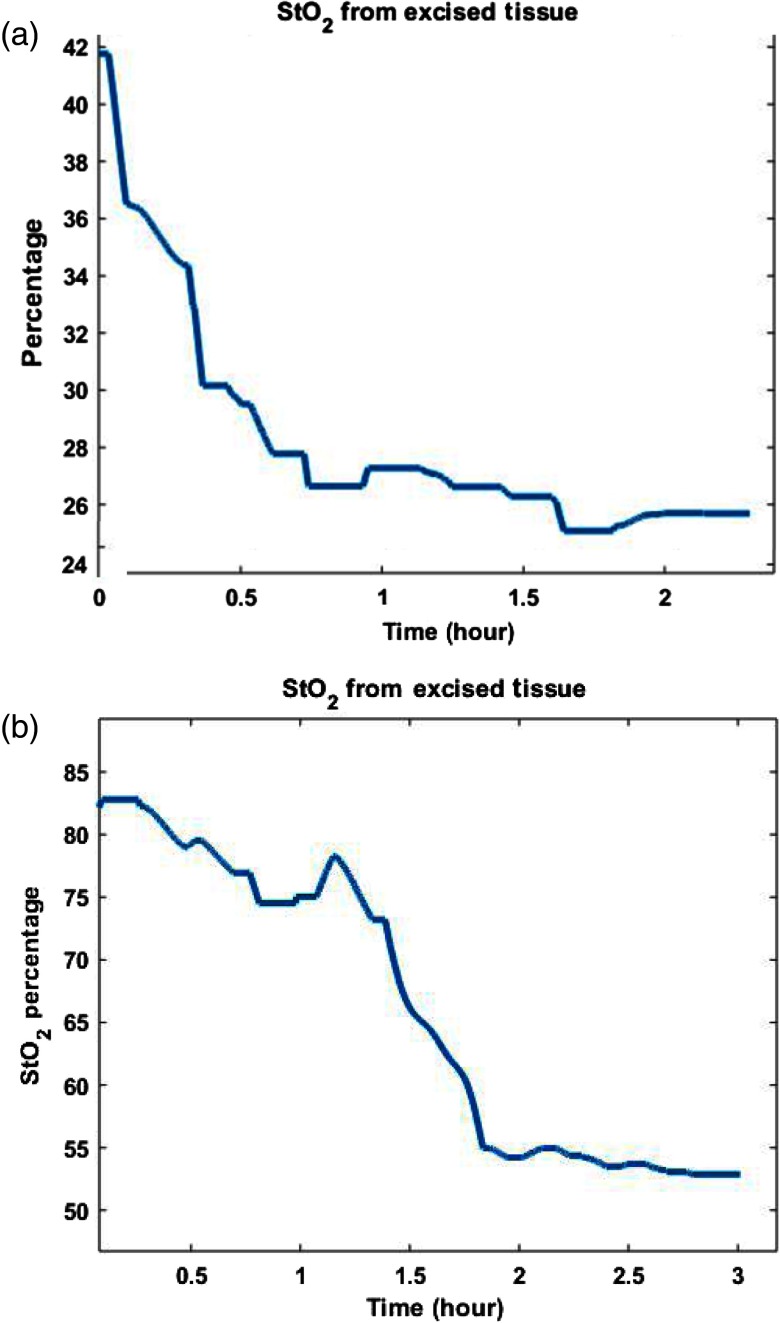
Free tissue transfer (FTT) surgery for breast reconstruction following mastectomy has become a routine operation with high success rates. Although failure is low, it can have a devastating impact on patient recovery, prognosis, and psychological well-being. Continuous and objective monitoring of tissue oxygen saturation (StO2) has been shown to reduce failure rates through rapid detection time of postoperative vascular complications. We have developed a pervasive wearable wireless device that employs near-infrared spectroscopy (NIRS) to continuously monitor FTT via StO2 measurement. Previously tested on different models, the results of a clinical study are introduced. Our goal for the study is to demonstrate that the developed device can reliably detect StO2 variations in a clinical setting: 14 patients were recruited. Advanced data analysis was performed on the StO2 variations, the relative StO2 gradient change, and the classification of the StO2 within different clusters of blood occlusion level (from 0% to 100% at 25% step) based on previous studies made on a vascular phantom and animals. The outcomes of the clinical study concur with previous experimental results and the expected biological responses. This suggests that the device is able to correctly detect perfusion changes and provide real-time assessment on the viability of the FTT in a clinical setting.
Keywords: breast reconstruction surgery; free tissue transfer; internet of things; near-infrared spectroscopy; spectroscopy; wearable device.
Figures
References
-
- Berthelot M., et al. , “Wireless wearable self-calibrated sensor for perfusion assessment of myocutaneous tissue,” in IEEE 13th Int. Conf. Wearable and Implantable Body Sensor Networks (BSN), IEEE, pp. 171–176 (2016).
-
- Sinis N., et al. , “Free flap monitoring with continuous tissue oxygen tension measurement,” Eur. J. Plastic Surg. 28(8), 507–512 (2006).10.1007/s00238-006-0032-7 - DOI
