

Dynamic right ventricular-pulmonary arterial uncoupling during maximum incremental exercise in exercise pulmonary hypertension and pulmonary arterial hypertension
- PMID: 31218910
- PMCID: PMC6643191
- DOI: 10.1177/2045894019862435
Dynamic right ventricular-pulmonary arterial uncoupling during maximum incremental exercise in exercise pulmonary hypertension and pulmonary arterial hypertension
Abstract
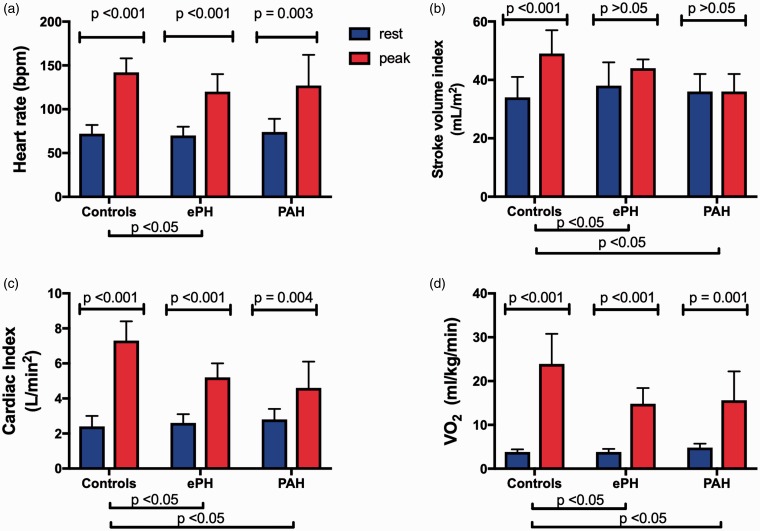
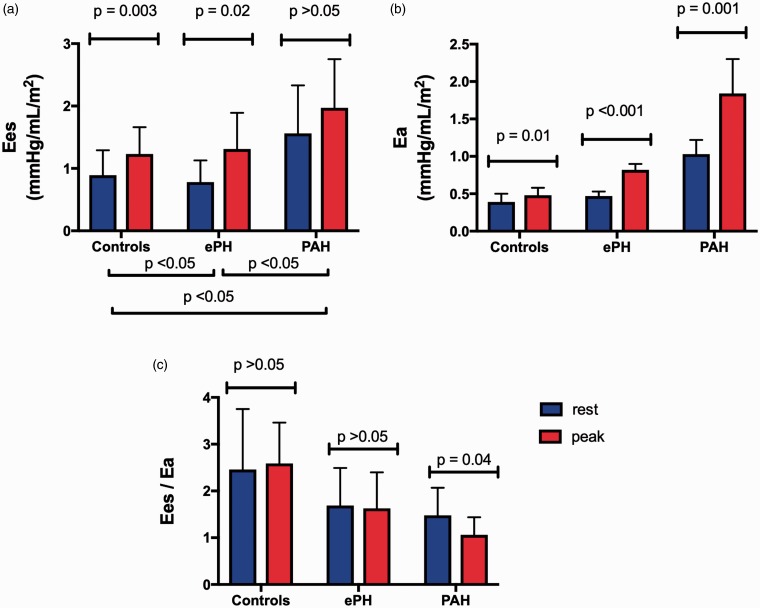
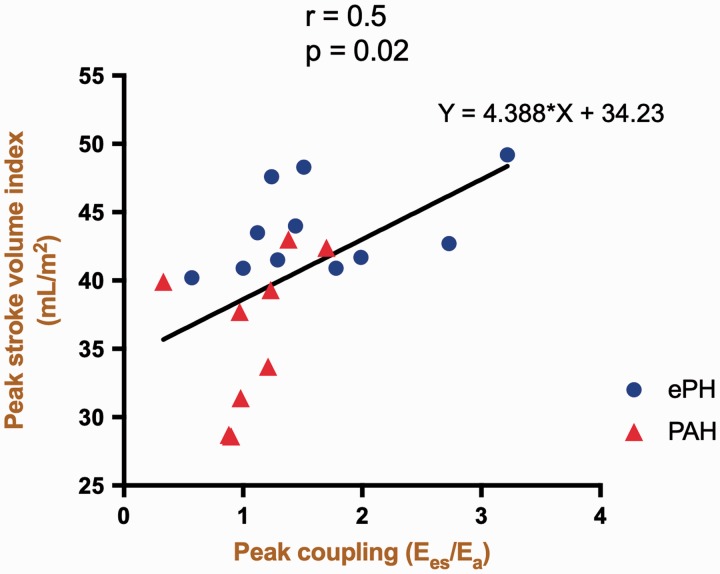
Despite recent advances, the prognosis of pulmonary hypertension (PH) remains poor. While the initial insult in PH implicates the pulmonary vasculature, the functional state, exercise capacity, and survival of such patients are closely linked to right ventricular (RV) function. In the current study, we sought to investigate the effects of maximum incremental exercise on the matching of RV contractility and afterload (i.e. right ventricular-pulmonary arterial [RV-PA] coupling) in patients with exercise PH (ePH) and pulmonary arterial hypertension (PAH). End-systolic elastance (Ees), pulmonary arterial elastance (Ea), and RV-PA coupling (Ees/Ea) were determined using single-beat pressure-volume loop analysis in 40 patients that underwent maximum invasive cardiopulmonary exercise testing. Eleven patients had ePH, nine had PAH, and 20 were age-matched controls. During exercise, the impaired exertional contractile reserve in PAH was associated with blunted stroke volume index (SVI) augmentation and reduced peak oxygen consumption (peak VO2 %predicted). Compared to PAH, ePH demonstrated increased RV contractility in response to increasing RV afterload during exercise; however, this was insufficient and resulted in reduced peak RV-PA coupling. The dynamic RV-PA uncoupling in ePH was associated with similarly blunted SVI augmentation and peak VO2 as PAH. In conclusion, dynamic rest-to-peak exercise RV-PA uncoupling during maximum exercise blunts SV increase and reduces exercise capacity in exercise PH and PAH. In ePH, the insufficient increase in RV contractility to compensate for increasing RV afterload during maximum exercise leads to deterioration of RV-PA coupling. These data provide evidence that even in the early stages of PH, RV function is compromised.
Keywords: exercise pulmonary hypertension; pulmonary arterial hypertension; right ventricular–pulmonary arterial coupling.
Figures
Similar articles
-
Sex-Related Differences in Dynamic Right Ventricular-Pulmonary Vascular Coupling in Heart Failure With Preserved Ejection Fraction.Chest. 2021 Jun;159(6):2402-2416. doi: 10.1016/j.chest.2020.12.028. Epub 2021 Jan 1. Chest. 2021. PMID: 33388286
-
Right Ventricular-Arterial Uncoupling During Exercise in Heart Failure With Preserved Ejection Fraction: Role of Pulmonary Vascular Dysfunction.Chest. 2019 Nov;156(5):933-943. doi: 10.1016/j.chest.2019.04.109. Epub 2019 May 16. Chest. 2019. PMID: 31103695
-
The effects of exercise on right ventricular contractility and right ventricular-arterial coupling in pulmonary hypertension.Am J Respir Crit Care Med. 2015 May 1;191(9):1050-7. doi: 10.1164/rccm.201412-2271OC. Am J Respir Crit Care Med. 2015. PMID: 25710636 Clinical Trial.
-
Assessing Right Ventricle Pulmonary Artery Coupling and Uncoupling Using Echocardiography and Cardiopulmonary Exercise Test in Post Operative TOF Patients.Curr Probl Cardiol. 2023 Aug;48(8):101214. doi: 10.1016/j.cpcardiol.2022.101214. Epub 2022 Apr 20. Curr Probl Cardiol. 2023. PMID: 35460685 Review.
-
Right ventricular function in pulmonary (arterial) hypertension.Herz. 2019 Sep;44(6):509-516. doi: 10.1007/s00059-019-4815-6. Herz. 2019. PMID: 31101945 Review. English.
Cited by
-
Poor cardiac output reserve in pulmonary arterial hypertension is associated with right ventricular stiffness and impaired interventricular dependence.Eur Respir J. 2024 Jul 18;64(1):2400420. doi: 10.1183/13993003.00420-2024. Print 2024 Jul. Eur Respir J. 2024. PMID: 38843915 Free PMC article.
-
High Right Ventricular Afterload during Exercise in Patients with Pulmonary Arterial Hypertension.J Clin Med. 2021 May 9;10(9):2024. doi: 10.3390/jcm10092024. J Clin Med. 2021. PMID: 34065097 Free PMC article. Review.
-
New echocardiographic indices of shift to biventricular failure to optimize risk stratification of chronic heart failure.ESC Heart Fail. 2022 Feb;9(1):476-485. doi: 10.1002/ehf2.13722. Epub 2021 Dec 7. ESC Heart Fail. 2022. PMID: 34874122 Free PMC article.
-
Role of Exercise in Pulmonary Hypertension: Evidence from Bench to Bedside.Pulse (Basel). 2024 Jun 5;12(1):66-75. doi: 10.1159/000539537. eCollection 2024 Jan-Dec. Pulse (Basel). 2024. PMID: 39022559 Free PMC article. Review.
-
The Current Role of Cardiopulmonary Exercise Test in the Diagnosis and Management of Pulmonary Hypertension.J Clin Med. 2023 Aug 23;12(17):5465. doi: 10.3390/jcm12175465. J Clin Med. 2023. PMID: 37685532 Free PMC article. Review.
References
-
- Forfia PR, Fisher MR, Mathai SC, et al. Tricuspid annular displacement predicts survival in pulmonary hypertension. Am J Respir Crit Care Med 2006; 174: 1034–1041. - PubMed
-
- D’Alonzo GE, Barst RJ, Ayres SM, et al. Survival in patients with primary pulmonary hypertension. Results from a national prospective registry. Ann Intern Med 1991; 115: 343–349. - PubMed
-
- Benza RL, Miller DP, Barst RJ, et al. An evaluation of long-term survival from time of diagnosis in pulmonary arterial hypertension from the REVEAL Registry. Chest 2012; 142: 448–456. - PubMed
-
- Badesch DB, Raskob GE, Elliott CG, et al. Pulmonary arterial hypertension: baseline characteristics from the REVEAL Registry. Chest 2010; 137: 376–387. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
Miscellaneous
