

The Pitt Bacteremia Score Predicts Mortality in Nonbacteremic Infections
- PMID: 31219148
- PMCID: PMC7156778
- DOI: 10.1093/cid/ciz528
The Pitt Bacteremia Score Predicts Mortality in Nonbacteremic Infections
Abstract
Background: Predicting mortality risk in patients is important in research settings. The Pitt bacteremia score (PBS) is commonly used as a predictor of early mortality risk in patients with bloodstream infections (BSIs). We determined whether the PBS predicts 14-day inpatient mortality in nonbacteremia carbapenem-resistant Enterobacteriaceae (CRE) infections.
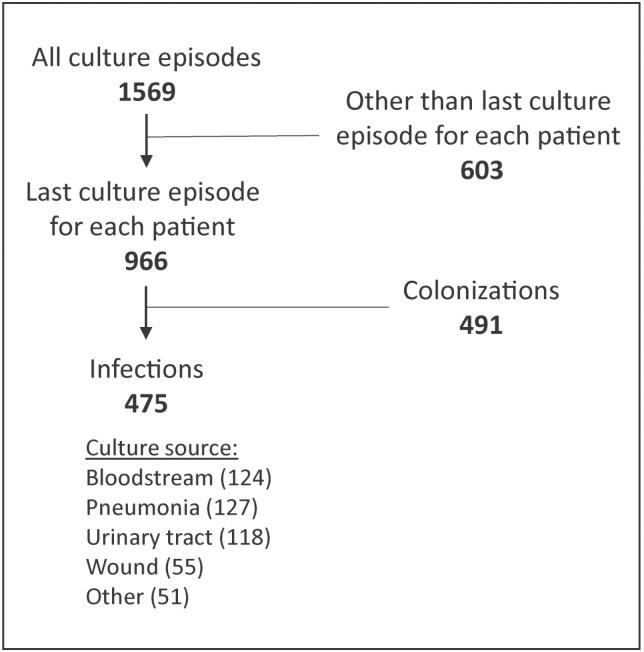
Methods: Patients were selected from the Consortium on Resistance Against Carbapenems in Klebsiella and Other Enterobacteriaceae, a prospective, multicenter, observational study. We estimated risk ratios to analyze the predictive ability of the PBS overall and each of its components individually. We analyzed each component of the PBS in the prediction of mortality, assessed the appropriate cutoff value for the dichotomized score, and compared the predictive ability of the qPitt score to that of the PBS.
Results: In a cohort of 475 patients with CRE infections, a PBS ≥4 was associated with mortality in patients with nonbacteremia infections (risk ratio [RR], 21.9; 95% confidence interval [CI], 7.0, 68.8) and with BSIs (RR, 6.0; 95% CI, 2.5, 14.4). In multivariable analysis, the hypotension, mechanical ventilation, mental status, and cardiac arrest parameters of the PBS were independent risk factors for 14-day all-cause inpatient mortality. The temperature parameter as originally calculated for the PBS was not independently associated with mortality. However, a temperature <36.0°C vs ≥36°C was independently associated with mortality. A qPitt score ≥2 had similar discrimination as a PBS ≥4 in nonbacteremia infections.
Conclusions: Here, we validated that the PBS and qPitt score can be used as reliable predictors of mortality in nonbacteremia CRE infections.
Keywords: Klebsiella pneumoniae; Carbapenem-resistant Enterobacteriaceae; Pitt bacteremia score; mortality; risk score.
© The Author(s) 2019. Published by Oxford University Press for the Infectious Diseases Society of America. All rights reserved. For permissions, e-mail: journals.permissions@oup.com.
Figures


Comment in
-
Resilience of the Pitt Bacteremia Score: 3 Decades and Counting.Clin Infect Dis. 2020 Apr 15;70(9):1834-1836. doi: 10.1093/cid/ciz535. Clin Infect Dis. 2020. PMID: 31219546 No abstract available.
References
-
- World Health Organization. Antimicrobial resistance—global report on surveillance. Available at: http://www.who.int/drugresistance/documents/surveillancereport/en Accessed 1 December 2018.
-
- Kontopidou F, Giamarellou H, Katerelos P, et al. ; Group for the Study of KPC-Producing Klebsiella pneumoniae Infections in Intensive Care Units Infections caused by carbapenem-resistant Klebsiella pneumoniae among patients in intensive care units in Greece: a multi-centre study on clinical outcome and therapeutic options. Clin Microbiol Infect 2014; 20:O117–23. - PubMed
-
- Tumbarello M, Trecarichi EM, De Rosa FG, et al. ; ISGRI-SITA (Italian Study Group on Resistant Infections of the Società Italiana Terapia Antinfettiva) Infections caused by KPC-producing Klebsiella pneumoniae: differences in therapy and mortality in a multicentre study. J Antimicrob Chemother 2015; 70:2133–43. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- R01 AI119446/AI/NIAID NIH HHS/United States
- UM1 AI104681/AI/NIAID NIH HHS/United States
- R01 AI072219/AI/NIAID NIH HHS/United States
- R01 AI104895/AI/NIAID NIH HHS/United States
- UL1 TR000439/TR/NCATS NIH HHS/United States
- R21 AI114508/AI/NIAID NIH HHS/United States
- S10 OD018164/OD/NIH HHS/United States
- P30 AI050410/AI/NIAID NIH HHS/United States
- R21 AI135522/AI/NIAID NIH HHS/United States
- R21 AI123747/AI/NIAID NIH HHS/United States
- UL1 TR002548/TR/NCATS NIH HHS/United States
- K24 AI093969/AI/NIAID NIH HHS/United States
- R01 AI063517/AI/NIAID NIH HHS/United States
- UL1 TR001863/TR/NCATS NIH HHS/United States
- R01 AI100560/AI/NIAID NIH HHS/United States
