

Increased mortality risk associated with serum sodium variations and borderline hypo- and hypernatremia in hospitalized adults
- PMID: 31219584
- PMCID: PMC7538236
- DOI: 10.1093/ndt/gfz098
Increased mortality risk associated with serum sodium variations and borderline hypo- and hypernatremia in hospitalized adults
Abstract
Background: This study aimed to evaluate short-term and long-term mortalities in a cohort of unselected hospitalized patients with serum sodium concentration ([Na+]) variations within and outside of reference range.
Methods: All adult patients admitted to the Mayo Clinic, Rochester, MN, USA from January 2011 to December 2013 (n = 147358) were retrospectively screened. Unique patients admitted during the study period were examined. The main exposure was serum [Na+] variation. Outcome measures were hospital and 1-year all-cause mortalities.
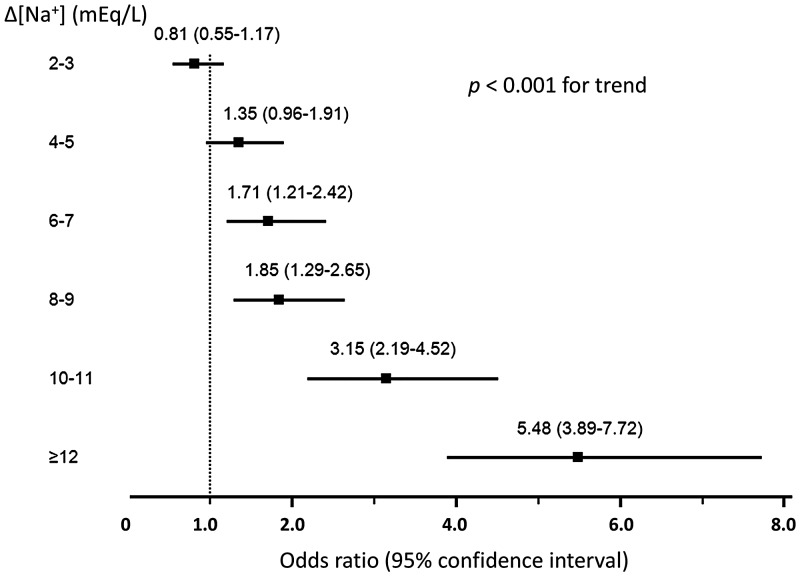
Results: A total of 60944 patients, mean age 63 ± 17 years, were studied. On admission, 17% (n = 10066) and 1.4% (n = 852) had hypo- and hypernatremia, respectively. During the hospital stay, 11044 and 4128 developed hypo- and hypernatremia, respectively, accounting for 52.3 and 82.9% of the total hypo- and hypernatremic patients. Serum [Na+] variations of ≥6 mEq/L occurred in 40.6% (n = 24 740) of the 60 944 patients and were significantly associated with hospital and 1-year mortalities after adjusting potential confounders (including demographics, comorbidities, estimated glomerular filtration rate, admission serum [Na+], number of [Na+] measurements and length of hospital stay). Adjusted odds ratios for hospital and 1-year mortalities increased with increasing [Na+] variations in a dose-dependent manner, from 1.47 to 5.48 (all 95% confidence intervals >1.0). Moreover, in fully adjusted models, [Na+] variations (≥6 mEq/L) within the reference range (135-145 mEq/L) or borderline hypo- or hypernatremia (133-137 and 143-147 mEq/L, respectively) compared with 138-142 mEq/L were associated with increased hospital and 1-year mortalities.
Conclusion: In hospitalized adults, [Na+] fluctuation (≥6 mEq/L) irrespective of admission [Na+] and borderline hypo- or hypernatremia are independent predictors of progressively increasing short- and long-term mortality burdens.
Keywords: borderline hypo- or hypernatremia; hypernatremia; hyponatremia; serum sodium ([Na+]) variation; short-term and long-term mortalities.
© The Author(s) 2019. Published by Oxford University Press on behalf of ERA-EDTA.
Figures
References
-
- Sajadieh A, Binici Z, Mouridsen MR. et al. Mild hyponatremia carries a poor prognosis in community subjects. Am J Med 2009; 122: 679–686 - PubMed
-
- Tsipotis E, Price LL, Jaber BL. et al. Hospital-associated hypernatremia spectrum and clinical outcomes in an unselected cohort. Am J Med 2018; 131: 72–82.e1 - PubMed
-
- Wald R, Jaber BL, Price LL. et al. Impact of hospital-associated hyponatremia on selected outcomes. Arch Intern Med 2010; 170: 294–302 - PubMed
-
- Kumar S, Berl T.. Sodium. Lancet 1998; 352: 220–228 - PubMed
