

Mutation Status of RAS, TP53, and SMAD4 is Superior to Mutation Status of RAS Alone for Predicting Prognosis after Resection of Colorectal Liver Metastases
- PMID: 31221662
- PMCID: PMC6774854
- DOI: 10.1158/1078-0432.CCR-19-0863
Mutation Status of RAS, TP53, and SMAD4 is Superior to Mutation Status of RAS Alone for Predicting Prognosis after Resection of Colorectal Liver Metastases
Abstract
Purpose: Somatic gene mutations have been increasingly recognized to impact prognosis following resection of colorectal liver metastases (CLM). We aimed to determine the impact of combinations of somatic mutations on survival in patients undergoing CLM resection.
Experimental design: We identified patients who underwent initial CLM resection during 2007-2017 and had genetic sequencing data available. Risk factors for overall survival (OS) and recurrence-free survival (RFS) were determined using Cox proportional hazards models.
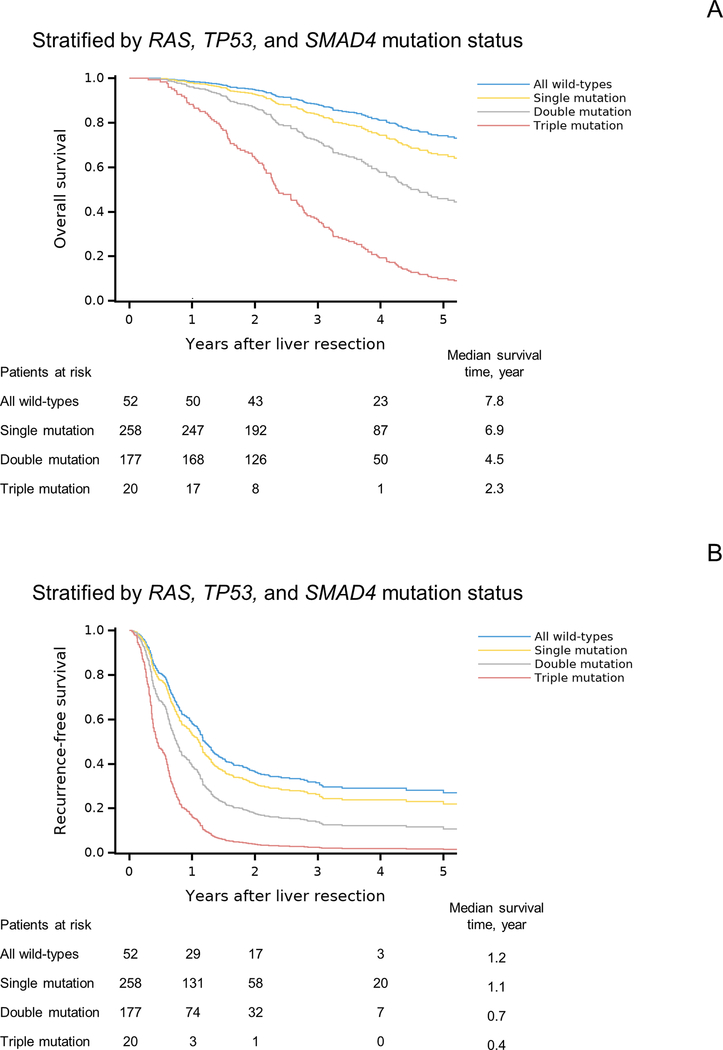
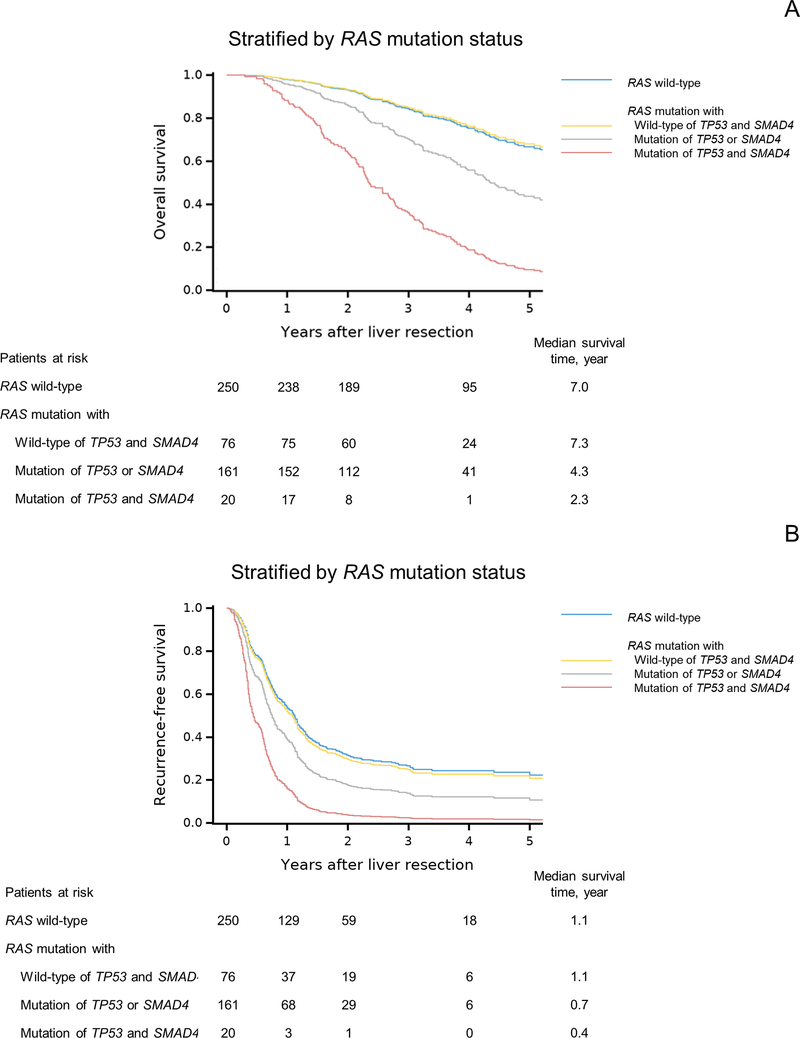
Results: Of 1460 patients who underwent CLM resection during the study period, 507 met the inclusion criteria. Multigene testing revealed mutation rates greater than 10% for TP53 (mutated in 70.8% of patients), APC (53.5%), RAS (50.7%), PIK3CA (15.8%), and SMAD4 (11.0%). BRAF was mutated in 2.0% of patients. BRAF, RAS, TP53, and SMAD4 mutations were significantly associated with OS, and RAS, TP53, and SMAD4 mutations were significantly associated with RFS. Coexisting mutations in RAS, TP53, and SMAD4 were associated with significantly worse OS and RFS than coexisting mutations in any 2 of these genes and mutations in 1 or none of these genes. Coexisting mutations in 2 genes conferred significantly worse OS and RFS than single mutation or no mutations. OS and RFS did not differ significantly between patients with RAS mutation and wild-type TP53 and SMAD4 and patients with wild-type RAS (P = 0.858 and 0.729, respectively).
Conclusions: RAS mutation status alone is not sufficient for precisely predicting prognosis after CLM resection.
©2019 American Association for Cancer Research.
Figures
References
-
- Nordlinger B, Guiguet M, Vaillant JC, Balladur P, Boudjema K, Bachellier P , et al. Surgical resection of colorectal carcinoma metastases to the liver. A prognostic scoring system to improve case selection, based on 1568 patients. Association Francaise de Chirurgie. Cancer 1996;77:1254–1262. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
