

Safety of a Restrictive versus Liberal Approach to Red Blood Cell Transfusion on the Outcome of AKI in Patients Undergoing Cardiac Surgery: A Randomized Clinical Trial
- PMID: 31221679
- PMCID: PMC6622429
- DOI: 10.1681/ASN.2019010004
Safety of a Restrictive versus Liberal Approach to Red Blood Cell Transfusion on the Outcome of AKI in Patients Undergoing Cardiac Surgery: A Randomized Clinical Trial
Abstract
Background: Safely reducing red blood cell transfusions can prevent transfusion-related adverse effects, conserve the blood supply, and reduce health care costs. Both anemia and red blood cell transfusion are independently associated with AKI, but observational data are insufficient to determine whether a restrictive approach to transfusion can be used without increasing AKI risk.
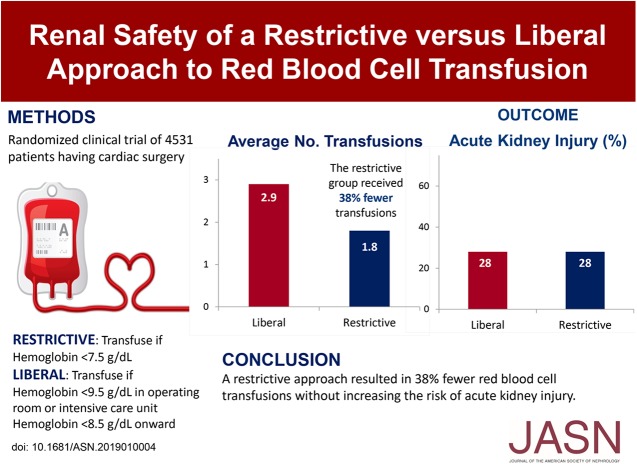
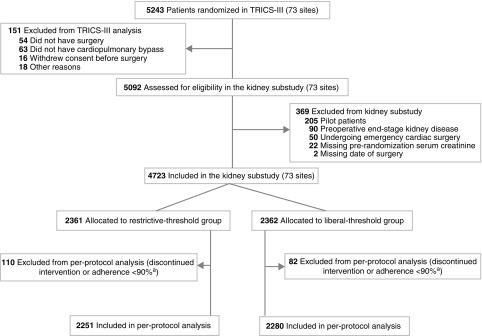
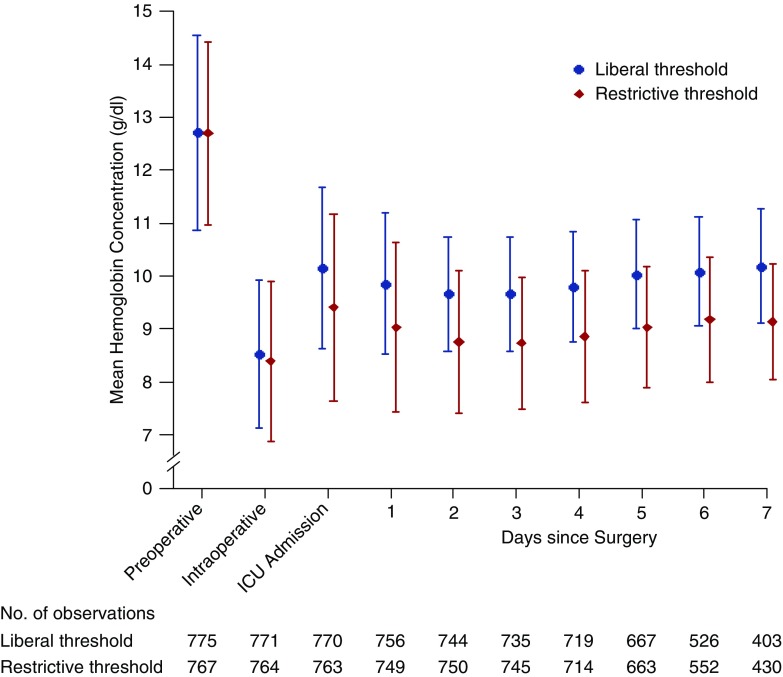
Methods: In a prespecified kidney substudy of a randomized noninferiority trial, we compared a restrictive threshold for red blood cell transfusion (transfuse if hemoglobin<7.5 g/dl, intraoperatively and postoperatively) with a liberal threshold (transfuse if hemoglobin<9.5 g/dl in the operating room or intensive care unit, or if hemoglobin<8.5 g/dl on the nonintensive care ward). We studied 4531 patients undergoing cardiac surgery with cardiopulmonary bypass who had a moderate-to-high risk of perioperative death. The substudy's primary outcome was AKI, defined as a postoperative increase in serum creatinine of ≥0.3 mg/dl within 48 hours of surgery, or ≥50% within 7 days of surgery.
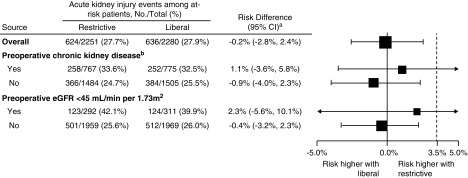
Results: Patients in the restrictive-threshold group received significantly fewer transfusions than patients in the liberal-threshold group (1.8 versus 2.9 on average, or 38% fewer transfusions in the restricted-threshold group compared with the liberal-threshold group; P<0.001). AKI occurred in 27.7% of patients in the restrictive-threshold group (624 of 2251) and in 27.9% of patients in the liberal-threshold group (636 of 2280). Similarly, among patients with preoperative CKD, AKI occurred in 33.6% of patients in the restrictive-threshold group (258 of 767) and in 32.5% of patients in the liberal-threshold group (252 of 775).
Conclusions: Among patients undergoing cardiac surgery, a restrictive transfusion approach resulted in fewer red blood cell transfusions without increasing the risk of AKI.
Keywords: Cardiac surgery; acute kidney injury; red blood cell transfusion.
Copyright © 2019 by the American Society of Nephrology.
Figures
Comment in
-
Restricting Red-Cell Transfusions in Cardiac Surgery: No Increase in AKI.J Am Soc Nephrol. 2019 Jul;30(7):1143-1144. doi: 10.1681/ASN.2019050509. Epub 2019 Jun 20. J Am Soc Nephrol. 2019. PMID: 31221680 Free PMC article. No abstract available.
References
-
- Vlaar APJ, Hofstra JJ, Determann RM, Veelo DP, Paulus F, Kulik W, et al. .: The incidence, risk factors, and outcome of transfusion-related acute lung injury in a cohort of cardiac surgery patients: A prospective nested case-control study. Blood 117: 4218–4225, 2011 - PubMed
-
- Delaney M, Wendel S, Bercovitz RS, Cid J, Cohn C, Dunbar NM, et al. .: Biomedical Excellence for Safer Transfusion (BEST) Collaborative : Transfusion reactions: Prevention, diagnosis, and treatment. Lancet 388: 2825–2836, 2016 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
