

Proliferating SPP1/MERTK-expressing macrophages in idiopathic pulmonary fibrosis
- PMID: 31221805
- PMCID: PMC8025672
- DOI: 10.1183/13993003.02441-2018
Proliferating SPP1/MERTK-expressing macrophages in idiopathic pulmonary fibrosis
Abstract
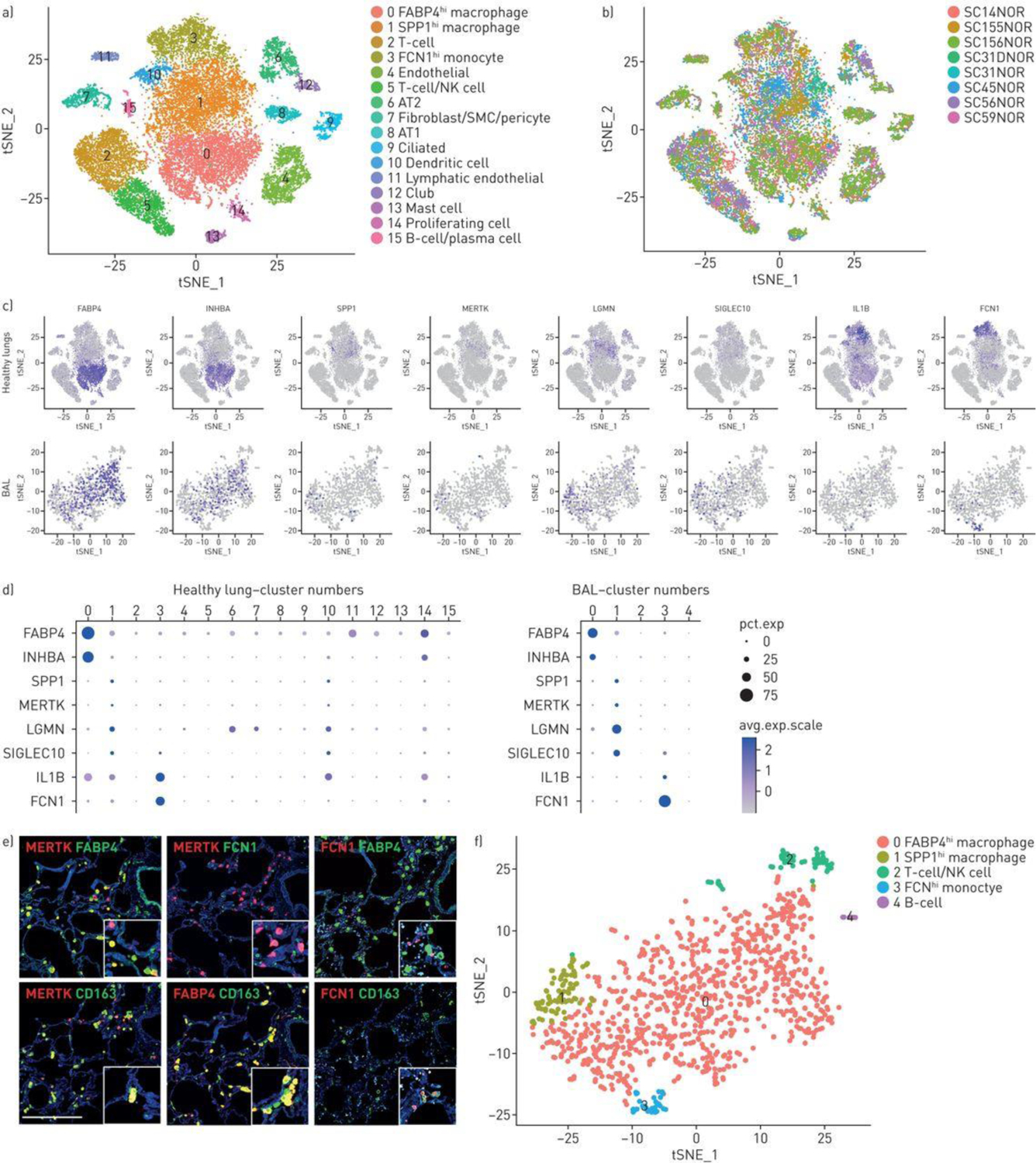
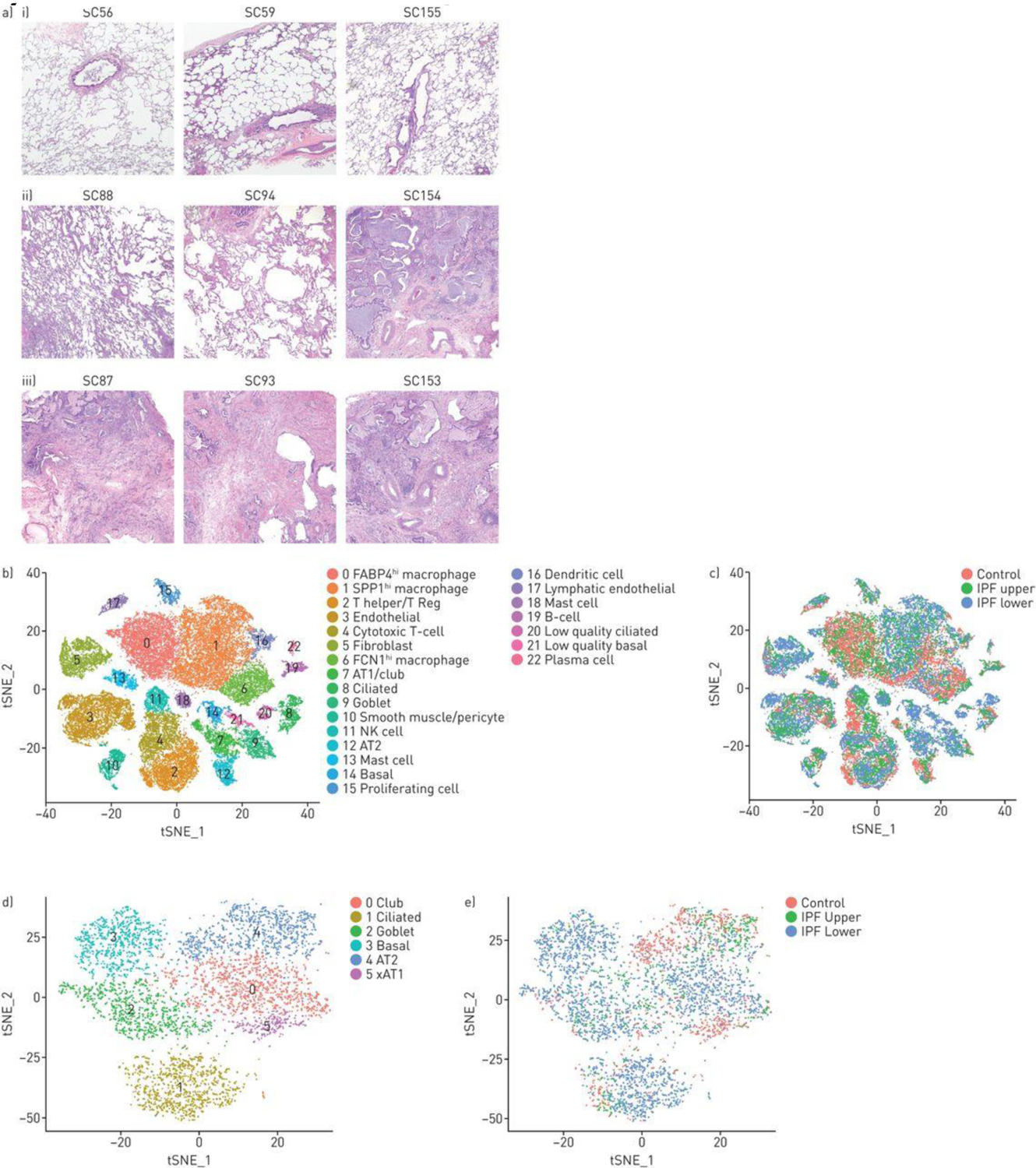
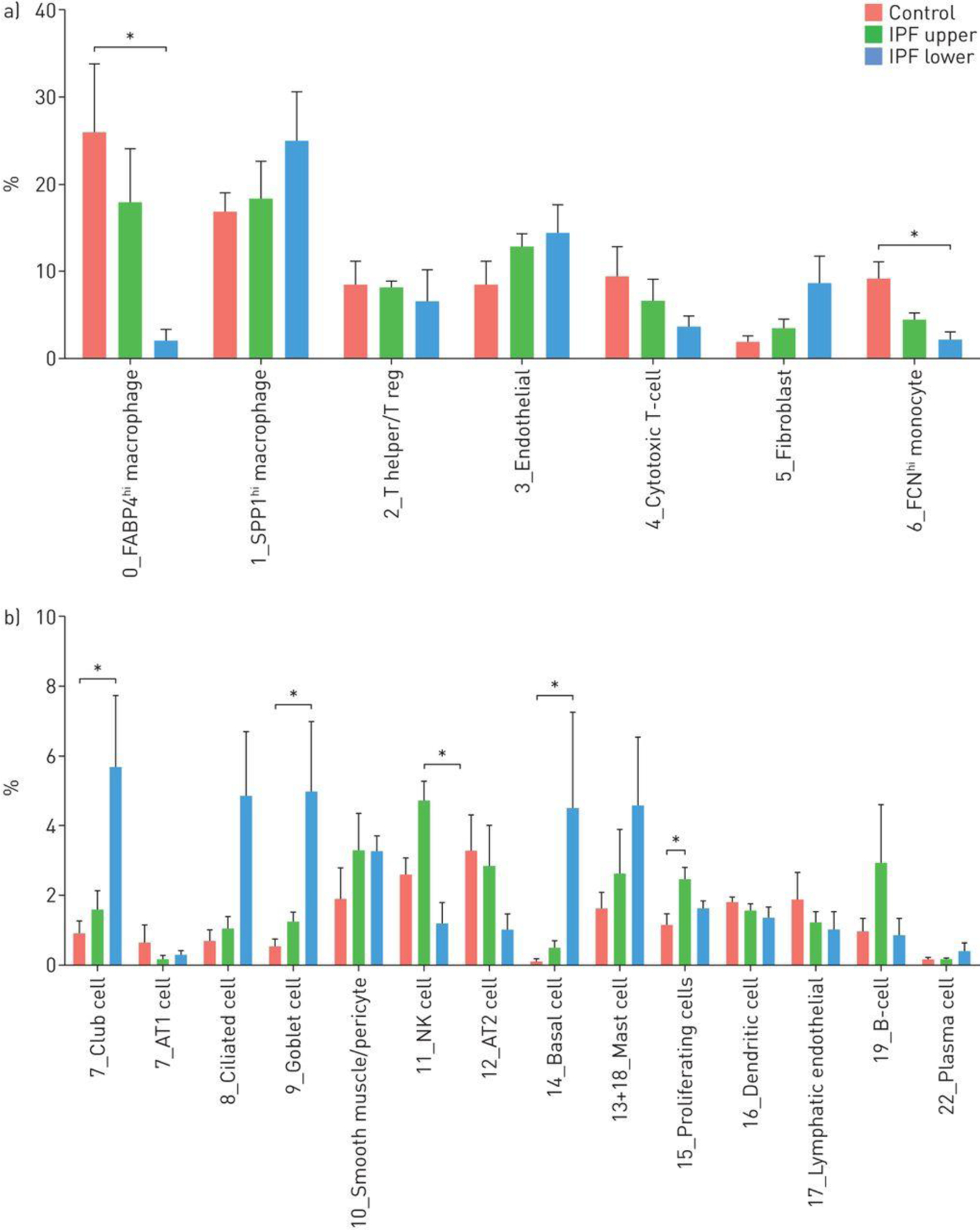
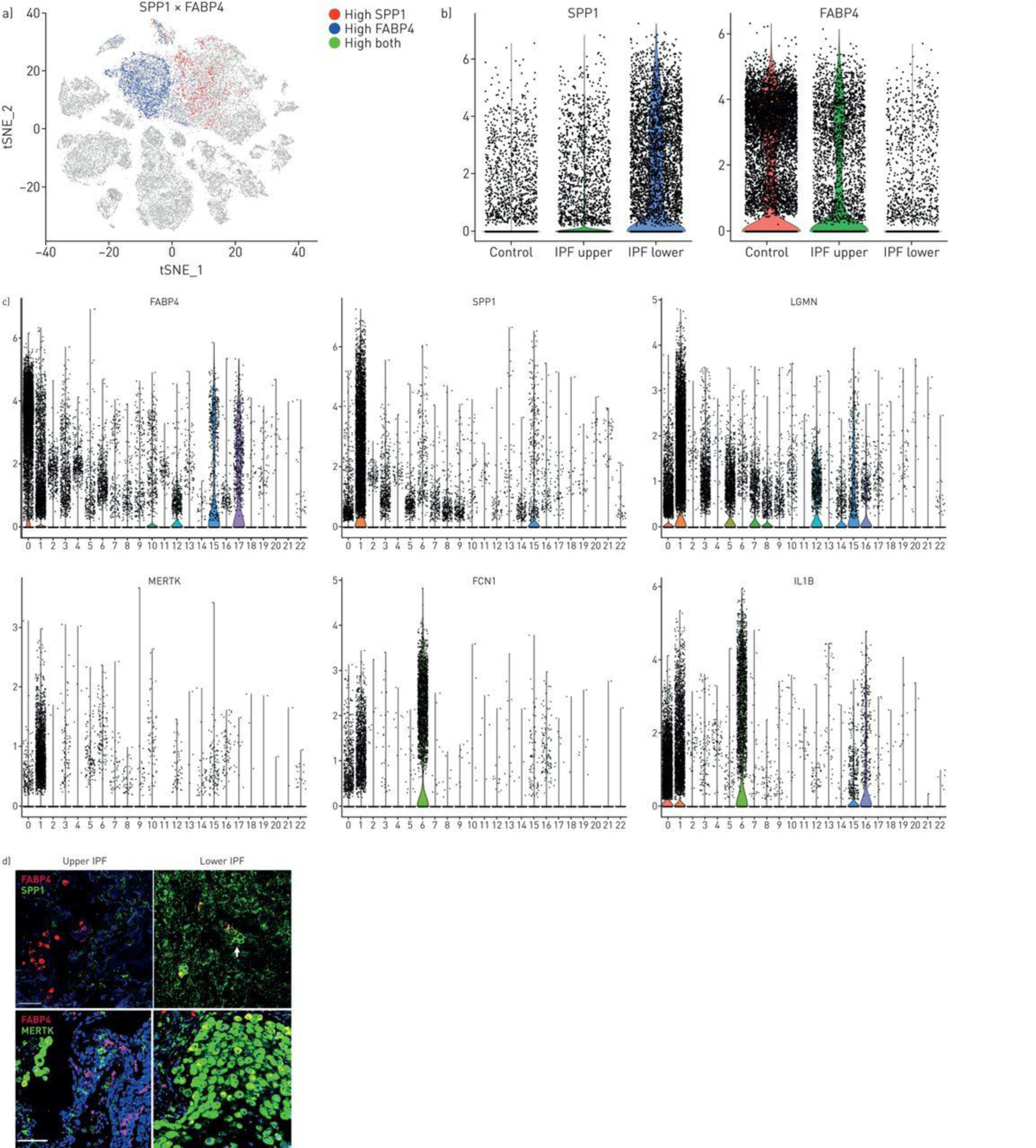
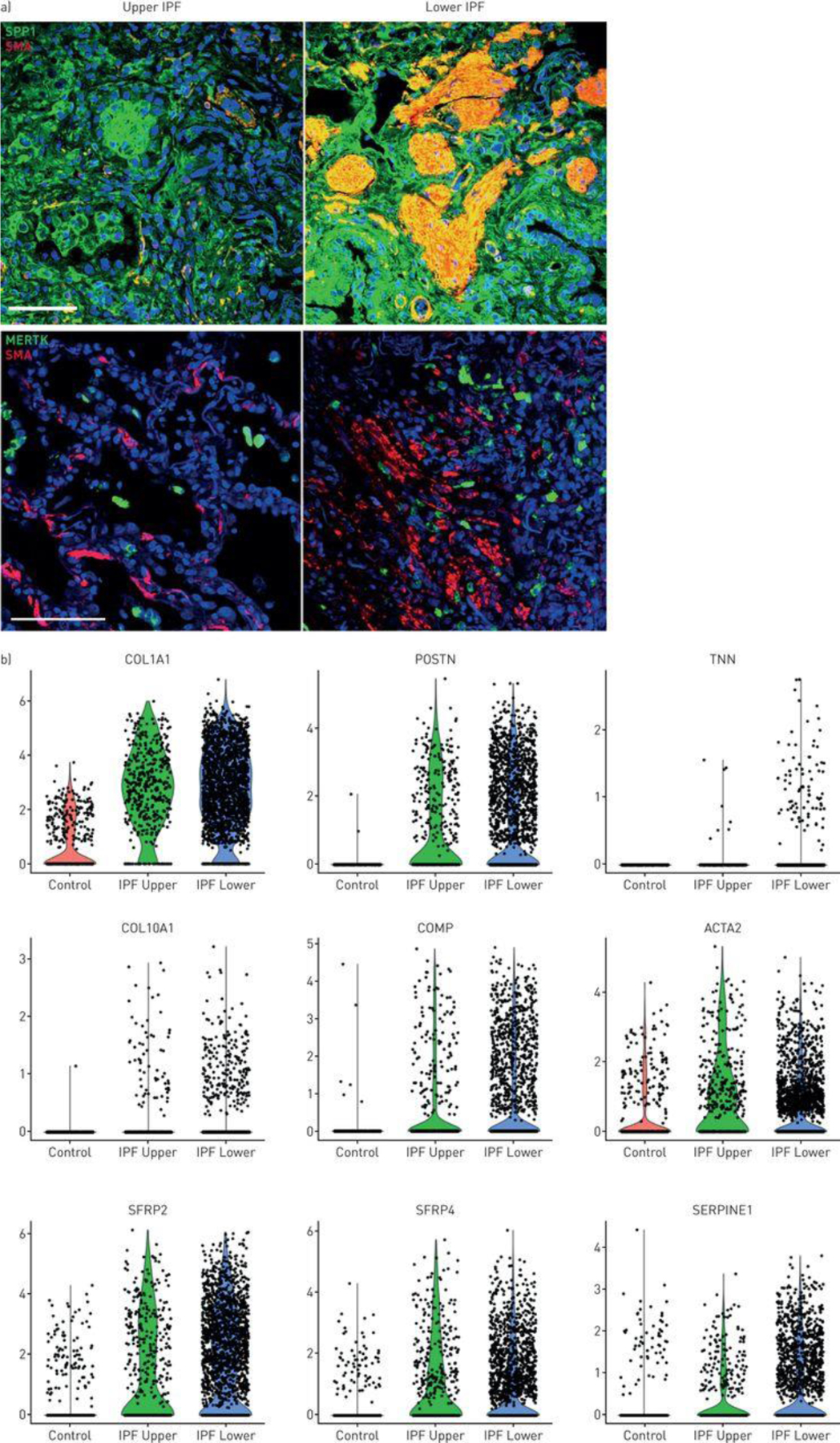
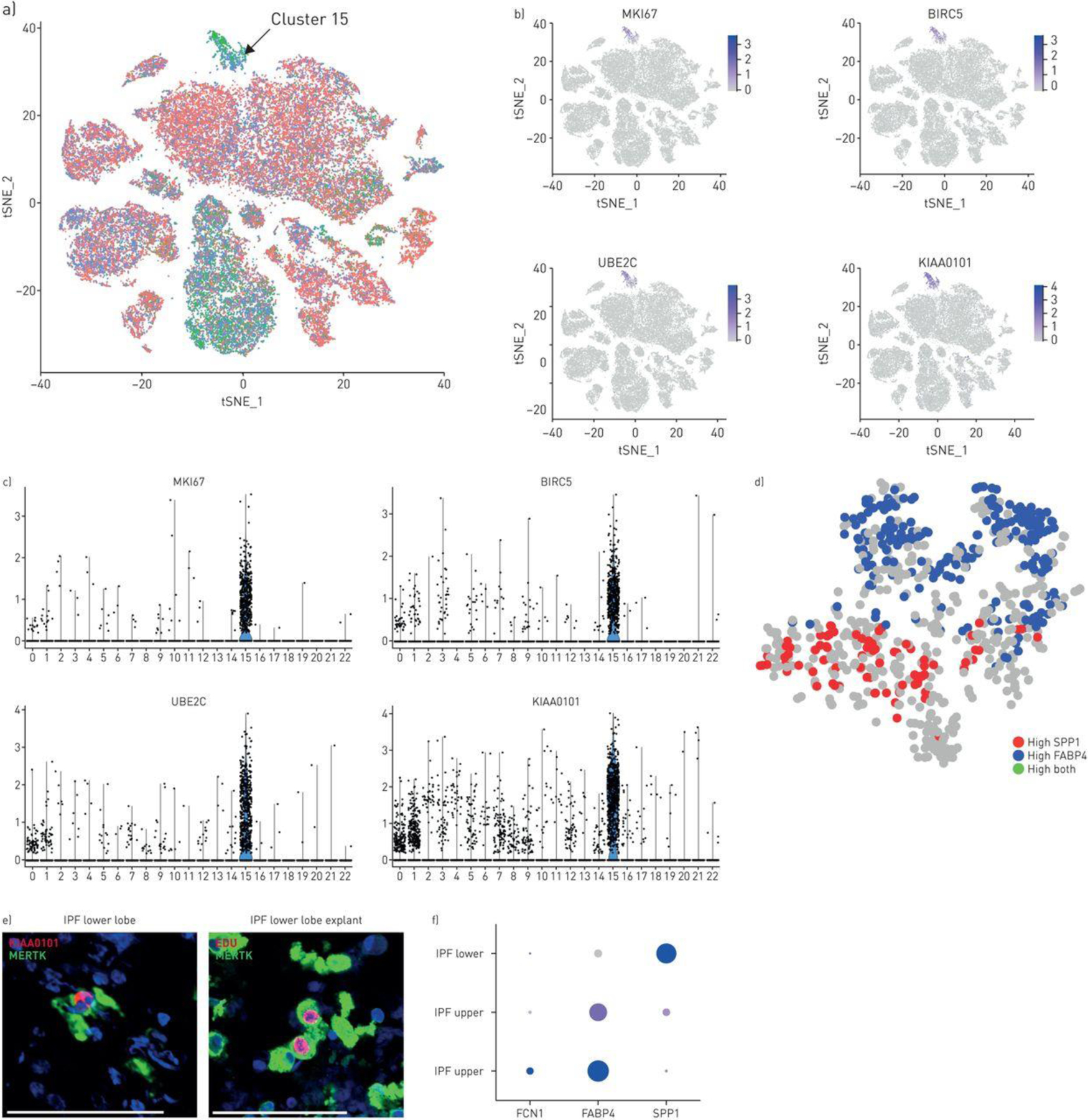
A comprehensive understanding of the changes in gene expression in cell types involved in idiopathic pulmonary fibrosis (IPF) will shed light on the mechanisms underlying the loss of alveolar epithelial cells and development of honeycomb cysts and fibroblastic foci. We sought to understand changes in IPF lung cell transcriptomes and gain insight into innate immune aspects of pathogenesis.We investigated IPF pathogenesis using single-cell RNA-sequencing of fresh lung explants, comparing human IPF fibrotic lower lobes reflecting late disease, upper lobes reflecting early disease and normal lungs.IPF lower lobes showed increased fibroblasts, and basal, ciliated, goblet and club cells, but decreased alveolar epithelial cells, and marked alterations in inflammatory cells. We found three discrete macrophage subpopulations in normal and fibrotic lungs, one expressing monocyte markers, one highly expressing FABP4 and INHBA (FABP4hi), and one highly expressing SPP1 and MERTK (SPP1hi). SPP1hi macrophages in fibrotic lower lobes showed highly upregulated SPP1 and MERTK expression. Low-level local proliferation of SPP1hi macrophages in normal lungs was strikingly increased in IPF lungs.Co-localisation and causal modelling supported the role for these highly proliferative SPP1hi macrophages in activation of IPF myofibroblasts in lung fibrosis. These data suggest that SPP1hi macrophages contribute importantly to lung fibrosis in IPF, and that therapeutic strategies targeting MERTK and macrophage proliferation may show promise for treatment of this disease.
Copyright ©ERS 2019.
Conflict of interest statement
Conflict of interest: C. Morse has nothing to disclose. Conflict of interest: T. Tabib has nothing to disclose. Conflict of interest: J. Sembrat has nothing to disclose. Conflict of interest: K. Buschur has nothing to disclose. Conflict of interest: H. Trejo Bittar has nothing to disclose. Conflict of interest: E. Valenzi has nothing to disclose. Conflict of interest: Y. Jiang has nothing to disclose. Conflict of interest: D.J. Kass reports grants from NIH, during the conduct of the study; grants from Regeneron, outside the submitted work. Conflict of interest: K. Gibson has nothing to disclose. Conflict of interest: W. Chen has nothing to disclose. Conflict of interest: A. Mora has nothing to disclose. Conflict of interest: P.V. Benos has nothing to disclose. Conflict of interest: M. Rojas has nothing to disclose. Conflict of interest: R. Lafyatis has nothing to disclose.
Figures
Comment in
-
Dysregulated balance of lung macrophage populations in idiopathic pulmonary fibrosis revealed by single-cell RNA seq: an unstable "ménage-à-trois".Eur Respir J. 2019 Aug 22;54(2):1901229. doi: 10.1183/13993003.01229-2019. Print 2019 Aug. Eur Respir J. 2019. PMID: 31439723 No abstract available.
References
-
- Blackwell TS, Tager AM, Borok Z, Moore BB, Schwartz DA, Anstrom KJ, Bar-Joseph Z, Bitterman P, Blackburn MR, Bradford W, Brown KK, Chapman HA, Collard HR, Cosgrove GP, Deterding R, Doyle R, Flaherty KR, Garcia CK, Hagood JS, Henke CA, Herzog E, Hogaboam CM, Horowitz JC, King TE Jr., Loyd JE, Lawson WE, Marsh CB, Noble PW, Noth I, Sheppard D, Olsson J, Ortiz LA, O’Riordan TG, Oury TD, Raghu G, Roman J, Sime PJ, Sisson TH, Tschumperlin D, Violette SM, Weaver TE, Wells RG, White ES, Kaminski N, Martinez FJ, Wynn TA, Thannickal VJ, Eu JP. Future directions in idiopathic pulmonary fibrosis research. An NHLBI workshop report. American journal of respiratory and critical care medicine 2014: 189(2): 214–222. - PMC - PubMed
-
- Sisson TH, Mendez M, Choi K, Subbotina N, Courey A, Cunningham A, Dave A, Engelhardt JF, Liu X, White ES, Thannickal VJ, Moore BB, Christensen PJ, Simon RH. Targeted injury of type II alveolar epithelial cells induces pulmonary fibrosis. American journal of respiratory and critical care medicine 2010: 181(3): 254–263. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
Research Materials
Miscellaneous