

Randomised clinical trial of ferric citrate hydrate on anaemia management in haemodialysis patients with hyperphosphataemia: ASTRIO study
- PMID: 31222044
- PMCID: PMC6586649
- DOI: 10.1038/s41598-019-45335-4
Randomised clinical trial of ferric citrate hydrate on anaemia management in haemodialysis patients with hyperphosphataemia: ASTRIO study
Abstract
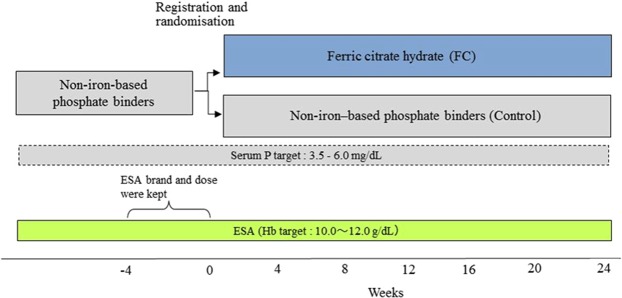
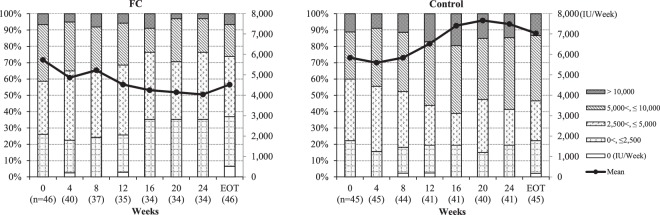
Ferric citrate hydrate (FC) is an iron-based phosphate binder approved for hyperphosphataemia in patients with chronic kidney disease. We conducted a randomised controlled trial to evaluate the effects of FC on anaemia management in haemodialysis patients with hyperphosphataemia. We 1:1 randomised 93 patients who were undergoing haemodialysis and being treated with non-iron-based phosphate binders and erythropoiesis-stimulating agents (ESA) to receive 24 weeks of FC or to continue their non-iron-based phosphate binders (control) in a multicentre, open-label, parallel-design. Phosphate level was controlled within target range (3.5-6.0 mg/dL). The primary endpoint was change in ESA dose from baseline to end of treatment. Secondary endpoints were changes in red blood cell, iron and mineral, and bone-related parameters. Compared with control, FC reduced ESA dose [mean change (SD), -1211.8 (3609.5) versus +1195 (6662.8) IU/week; P = 0.03] without significant differences in haemoglobin. FC decreased red blood cell distribution width (RDW) compared with control. While there were no changes in serum phosphate, FC reduced C-terminal fibroblast growth factor (FGF) 23 compared with control. The incidence of adverse events did not differ significantly between groups. Despite unchanged phosphate and haemoglobin levels, FC reduced ESA dose, RDW, and C-terminal FGF23 compared with control.
Conflict of interest statement
K.Y., M.F., T.A. and H.H. received consulting fees from Torii Pharmaceutical Co. Ltd. and Japan Tobacco, Inc. M.N. received research funding and consulting fees from Torii Pharmaceutical Co. Ltd. and Japan Tobacco, Inc. M.W. received consulting fees from Torii Pharmaceutical Co. Ltd. and Keryx Biopharmaceuticals, Inc. K.I. is an employee of Torii Pharmaceutical Co. Ltd. and K.H. is an employee of Japan Tobacco Inc. The study was conducted by the funding from Torii Pharmaceutical Co., Ltd. (Tokyo, Japan) and Japan Tobacco Inc. (Tokyo, Japan).
Figures


References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
