

Detecting inflammation in rheumatoid arthritis using Fourier transform analysis of dorsal optical transmission images from a pilot study
- PMID: 31222990
- PMCID: PMC6977034
- DOI: 10.1117/1.JBO.24.6.066008
Detecting inflammation in rheumatoid arthritis using Fourier transform analysis of dorsal optical transmission images from a pilot study
Abstract
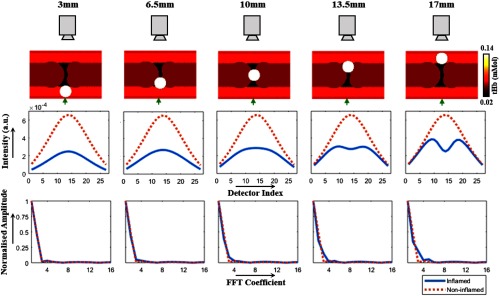
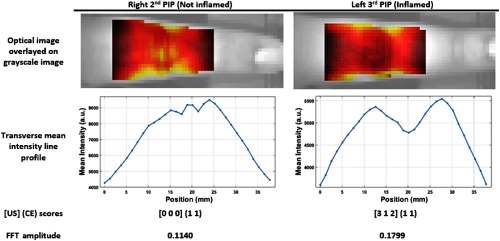
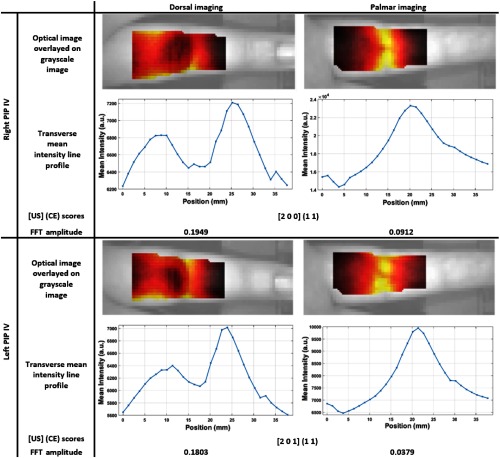
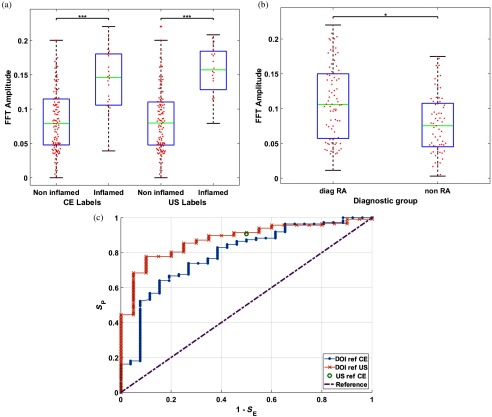
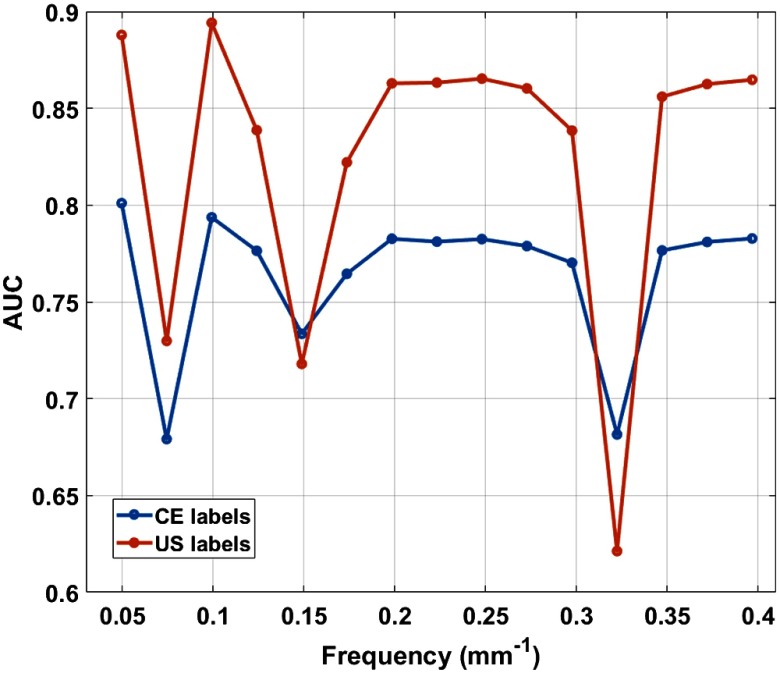
A clinical need exists for low-cost and noninvasive imaging tools capable of detecting inflammation in the joints of inflammatory arthritis patients. Previous studies have reported an optical contrast between inflamed and noninflamed joints resulting from distinct absorption and scattering properties. Accurate classification using nonocclusion-based continuous wave, transillumination imaging was limited to patient-specific changes during follow-up examination as opposed to single time-point examination, which was attributed to high intersubject variability. In distinction from previous work, optical images were acquired from the dorsal side with illumination on the palmar side and features about the spatial distribution of transmitted light along the joint were assessed using a normalized Fourier transform method. Results using this approach demonstrated an area under receiver operator curve of up to 0.888 for detecting inflammation in a pilot study involving single time-point examination of 144 joints from 21 rheumatology patients. This workflow may enable future development of clinically viable, low-cost devices for assessing inflammation in arthritis patients, without the need for cuff occlusion or comparison to baseline.
Keywords: intrinsic contrast; optical imaging; rheumatoid arthritis.
Figures
References
-
- National Audit Office, Services for People with Rheumatoid Arthritis, National Audit Office, Vol. 823, pp. 1–37 (2009).
-
- N. C. C. for Chronic Conditions et al., Rheumatoid Arthritis: National Clinical Guideline for Management and Treatment in Adults, Royal College of Physicians of London; (2009). - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
