

Study of epidemiological aspects of hyperuricemia in Poland
- PMID: 31225633
- PMCID: PMC8086669
- DOI: 10.5603/CJ.a2019.0034
Study of epidemiological aspects of hyperuricemia in Poland
Abstract
Background: The results of the latest epidemiological studies show that the problem of hyperuricemia affects many millions of people. The main purpose of the study was to assess the knowledge of physicians with regard to the epidemiology and treatment of hyperuricemia in Poland.
Methods: CAPI (computer assisted personal interview) interviews were conducted using short questionnaires among primary health care physicians, cardiologists and diabetologists. The entire questionnaire included 11 questions. Questions were asked to physicians at 5 different periods in time. The number of physicians surveyed, depended on the time period, and ranged from 8663 to 9980.
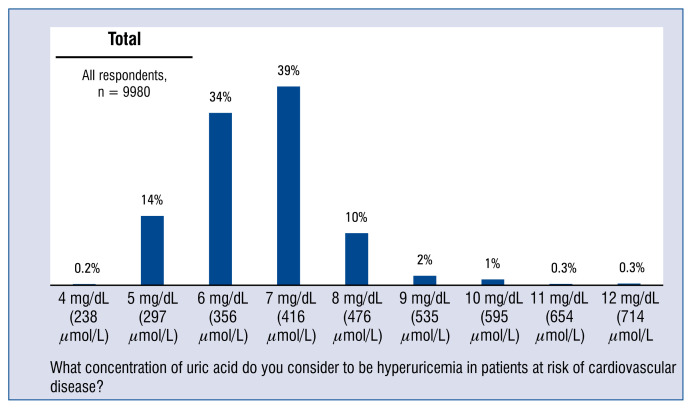
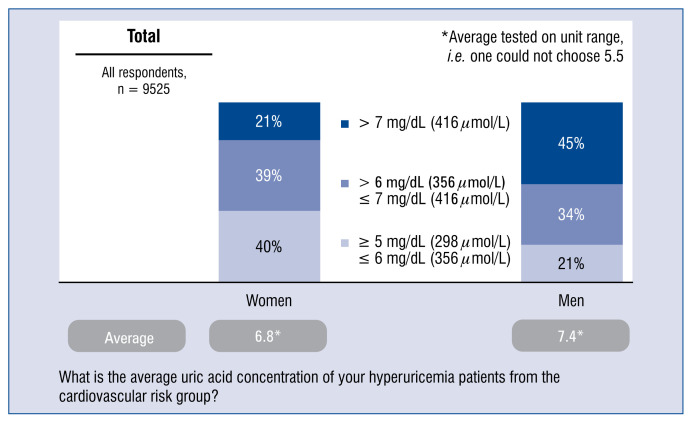
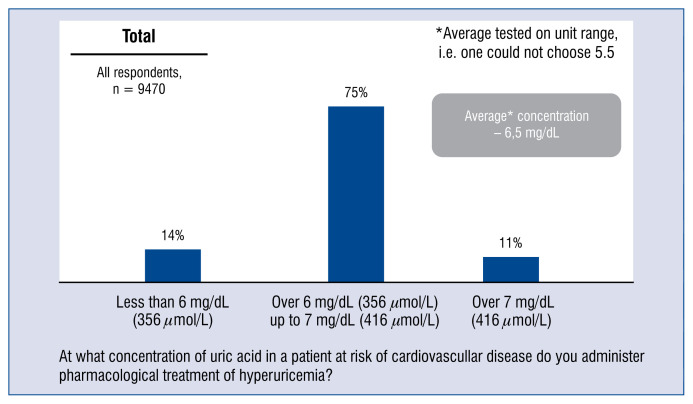
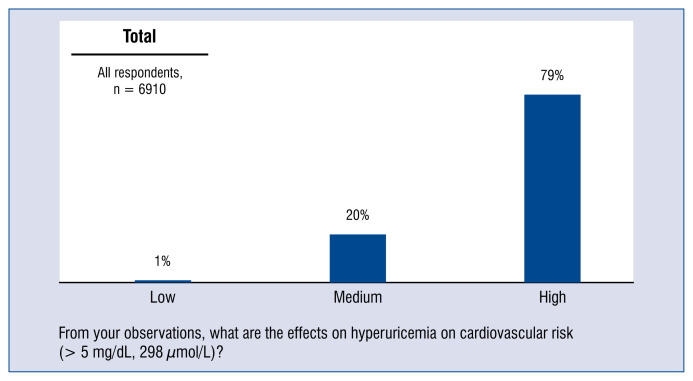
Results: Only every 1 in 7 physicians (14%) considered that hyperuricemia in patients with cardiovascular risk factors begins when the uric acid level is 5 mg/dL, thus in line with the expert recommendations. 72% of respondents asked to indicate the uric acid levels they consider to be indicative of hyperuricemia in patients in the cardiovascular risk group, gave values ranging from 6 to 7 mg/dL, namely the values justified in cases of a patient without such a risk, i.e. in the general population. 86% of doctors surveyed gave values different from that recommended by experts.
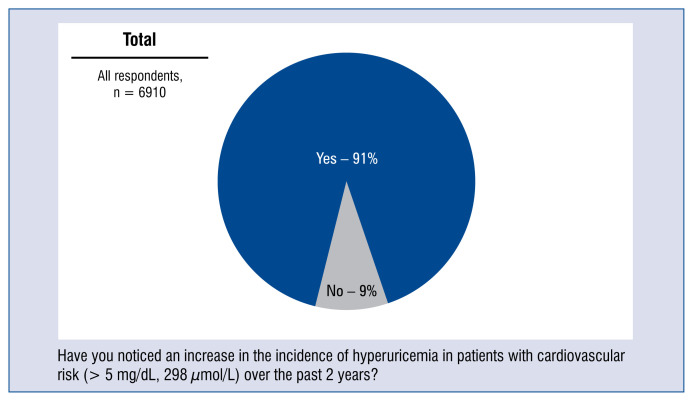
Conclusions: The findings of the questionnaire in this survey suggests that doctors often underestimate the problem of hyperuricemia in patients with a high risk of cardiovascular disease. An important step towards more effective therapy of hyperuricemia in routine clinical practice is to raise the awareness of hyperuricemia and its comorbidities both among doctors and patients and encourage monitoring and treatment.
Keywords: arterial hypertension; hyperuricemia.
Conflict of interest statement
Figures
Similar articles
-
How Are We Managing Patients with Hyperuricemia and Gout: A Cross Sectional Study Assessing Knowledge and Attitudes of Primary Care Physicians?Int J Environ Res Public Health. 2021 Jan 30;18(3):1234. doi: 10.3390/ijerph18031234. Int J Environ Res Public Health. 2021. PMID: 33573113 Free PMC article.
-
Knowledge and practice in the management of asymptomatic hyperuricemia among primary health care physicians in Jeddah, Western Region of Saudi Arabia.Saudi Med J. 2018 Dec;39(12):1218-1225. doi: 10.15537/smj.2018.12.23715. Saudi Med J. 2018. PMID: 30520504 Free PMC article.
-
An Assessment of Knowledge, Attitude, and Practices of Physicians in the Management of Hyperuricemia in India: A Questionnaire-Based Study.J Assoc Physicians India. 2021 Apr;69(4):11-12. J Assoc Physicians India. 2021. PMID: 34470189
-
[Hyperuricemia - more than gout : Impact on cardiovascular risk and renal insufficiency].Z Rheumatol. 2015 May;74(4):322-8. doi: 10.1007/s00393-014-1481-1. Z Rheumatol. 2015. PMID: 25962453 Review. German.
-
Hyperuricemia and Risk of Cardiovascular Outcomes: The Experience of the URRAH (Uric Acid Right for Heart Health) Project.High Blood Press Cardiovasc Prev. 2020 Apr;27(2):121-128. doi: 10.1007/s40292-020-00368-z. Epub 2020 Mar 10. High Blood Press Cardiovasc Prev. 2020. PMID: 32157643 Review.
Cited by
-
Resveratrol affects the expression of uric acid transporter by improving inflammation.Mol Med Rep. 2021 Aug;24(2):564. doi: 10.3892/mmr.2021.12203. Epub 2021 Jun 10. Mol Med Rep. 2021. PMID: 34109437 Free PMC article.
-
How Are We Managing Patients with Hyperuricemia and Gout: A Cross Sectional Study Assessing Knowledge and Attitudes of Primary Care Physicians?Int J Environ Res Public Health. 2021 Jan 30;18(3):1234. doi: 10.3390/ijerph18031234. Int J Environ Res Public Health. 2021. PMID: 33573113 Free PMC article.
-
Update on the epidemiology, genetics, and therapeutic options of hyperuricemia.Am J Transl Res. 2020 Jul 15;12(7):3167-3181. eCollection 2020. Am J Transl Res. 2020. PMID: 32774692 Free PMC article. Review.
-
Dietary pattern and risk of hyperuricemia: an updated systematic review and meta-analysis of observational studies.Front Nutr. 2024 Feb 28;11:1218912. doi: 10.3389/fnut.2024.1218912. eCollection 2024. Front Nutr. 2024. PMID: 38481974 Free PMC article. Review.
-
Knowledge, Attitudes, and Practices about Hyperuricemia and Gout in Community Health Workers and Patients with Diabetes.Healthcare (Basel). 2024 May 24;12(11):1072. doi: 10.3390/healthcare12111072. Healthcare (Basel). 2024. PMID: 38891147 Free PMC article.
References
-
- Freedman DS, Williamson DF, Gunter EW, et al. Relation of serum uric acid to mortality and ischemic heart disease. The NHANES I Epidemiologic Follow-up Study. Am J Epidemiol. 1995;141(7):637–644. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
