

Association of Mineralocorticoid Receptor Antagonist Use With All-Cause Mortality and Hospital Readmission in Older Adults With Acute Decompensated Heart Failure
- PMID: 31225889
- PMCID: PMC6593642
- DOI: 10.1001/jamanetworkopen.2019.5892
Association of Mineralocorticoid Receptor Antagonist Use With All-Cause Mortality and Hospital Readmission in Older Adults With Acute Decompensated Heart Failure
Abstract
Importance: Scarce data are available on the association of mineralocorticoid receptor antagonist (MRA) use with outcomes in acute decompensated heart failure (ADHF).
Objective: To investigate the association of MRA use with all-cause mortality and hospital readmission in patients with ADHF.
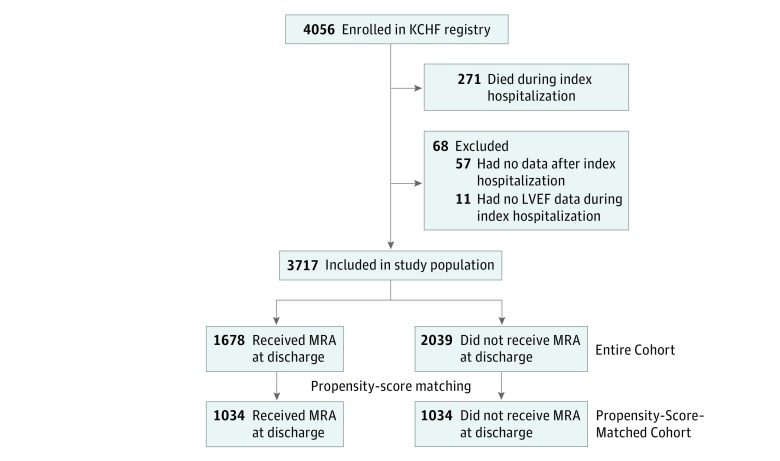
Design, setting, and participants: This cohort study examines participants enrolled in the Kyoto Congestive Heart Failure (KCHF) registry, a physician-initiated, prospective, multicenter cohort study of consecutive patients admitted for ADHF, between October 1, 2014, and March 31, 2016, into 1 of 19 secondary and tertiary hospitals throughout Japan. To balance the baseline characteristics associated with the selection of MRA use, a propensity score-matched cohort design was used, yielding 2068 patients. Data analysis was conducted from April to August 2018.
Exposures: Prescription of MRA at discharge from the index hospitalization.
Main outcomes and measures: Composite of all-cause death or heart failure hospitalization after discharge.
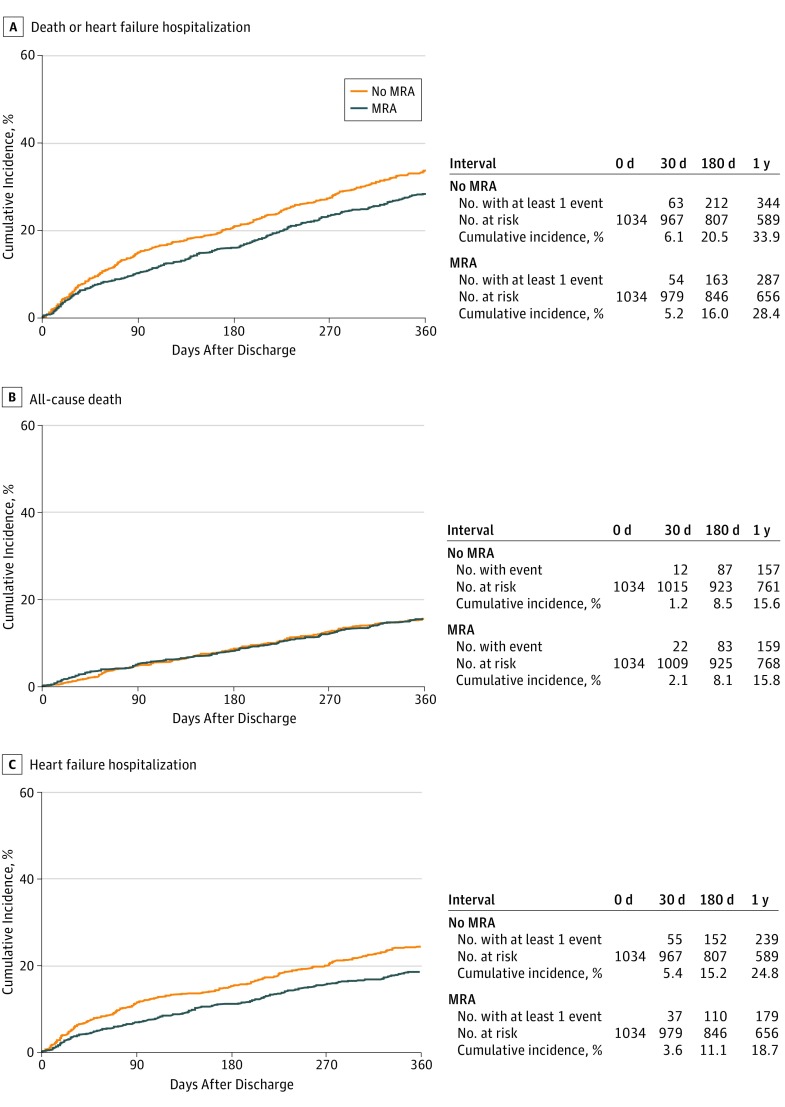
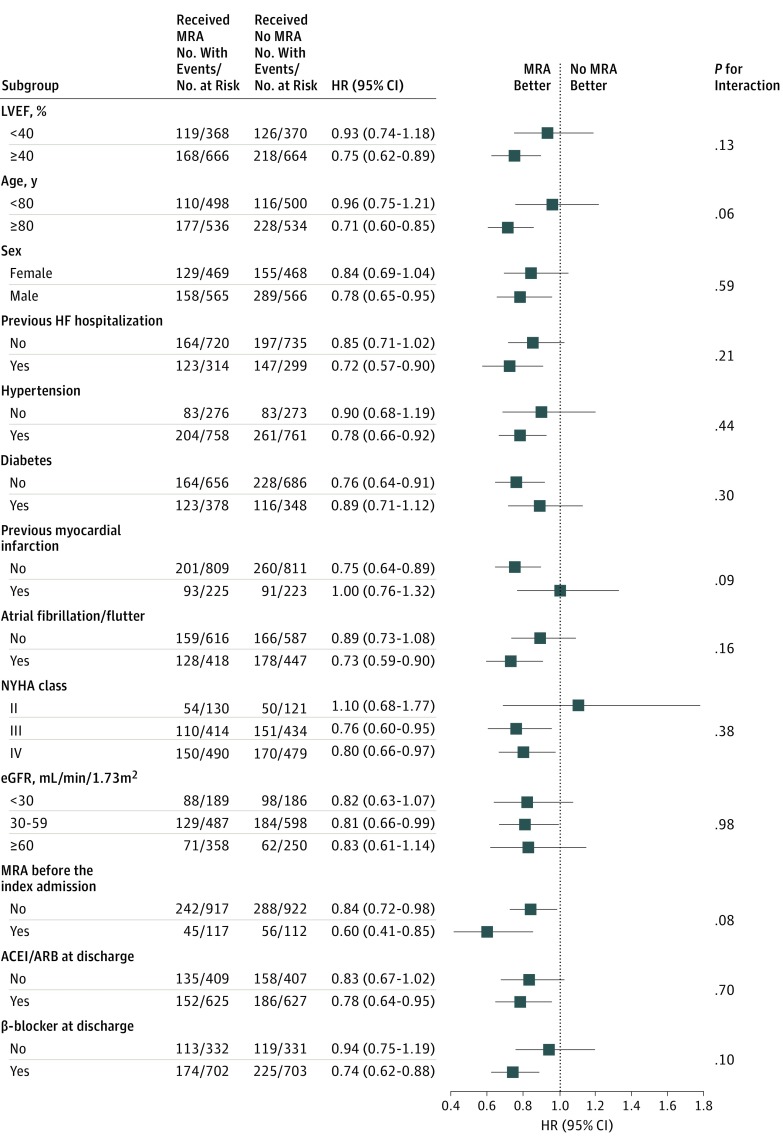
Results: Among 3717 patients hospitalized for ADHF, 1678 patients (45.1%) had received MRA at discharge and 2039 (54.9%) did not. After propensity score matching, 2068 patients (with a median [interquartile range] age of 80 [72-86] years, and of whom 937 [45.3%] were women) were included. In the matched cohort (n = 1034 in each group), the cumulative 1-year incidence of the primary outcome was statistically significantly lower in the MRA use group than in the no MRA use group (28.4% vs 33.9%; hazard ratio [HR], 0.81; 95% CI, 0.70-0.93; P = .003). Of the components of the primary outcome, the cumulative 1-year incidence of heart failure hospitalization was significantly lower in the MRA use group than in the no MRA use group (18.7% vs 24.8%; HR, 0.70; 95% CI, 0.60-0.86; P < .001), whereas no difference in mortality was found between the 2 groups (15.6% vs 15.8%; HR, 0.98; 95% CI, 0.82-1.18; P = .85). No difference in all-cause hospitalization was observed between the 2 groups (35.3% vs 38.2%; HR, 0.88; 95% CI, 0.77-1.01; P = .07). In additional analyses that stratified by left ventricular ejection fraction, the association of MRA use with the primary outcome was statistically significant in patients with left ventricular ejection fraction of 40% or greater.
Conclusions and relevance: Use of MRA at discharge from ADHF hospitalization did not appear to be associated with lower mortality but was associated with a lower risk of heart failure readmission. This finding suggests that MRA treatment at discharge may have minimal, if any, clinical advantages.
Conflict of interest statement
Figures
References
-
- Pitt B, Remme W, Zannad F, et al. ; Eplerenone Post-Acute Myocardial Infarction Heart Failure Efficacy and Survival Study Investigators . Eplerenone, a selective aldosterone blocker, in patients with left ventricular dysfunction after myocardial infarction. N Engl J Med. 2003;348(14):1309-1321. doi:10.1056/NEJMoa030207 - DOI - PubMed
