

Post-Discharge Services for Different Diagnoses Than Index Hospitalization Predict Decreased 30-Day Readmissions Among Medicare Beneficiaries
- PMID: 31228052
- PMCID: PMC6712241
- DOI: 10.1007/s11606-019-05115-2
Post-Discharge Services for Different Diagnoses Than Index Hospitalization Predict Decreased 30-Day Readmissions Among Medicare Beneficiaries
Abstract
Background: Efforts to reduce hospital readmissions include post-discharge interventions related to the illness treated during the index hospitalization (IH). These efforts may be inadequate because readmissions are precipitated by a wide range of health conditions unrelated to the primary diagnosis of the IH.
Objective: To investigate the relationship between post-discharge health services utilization for the same or a different diagnosis than the IH and unplanned 30-day readmission.
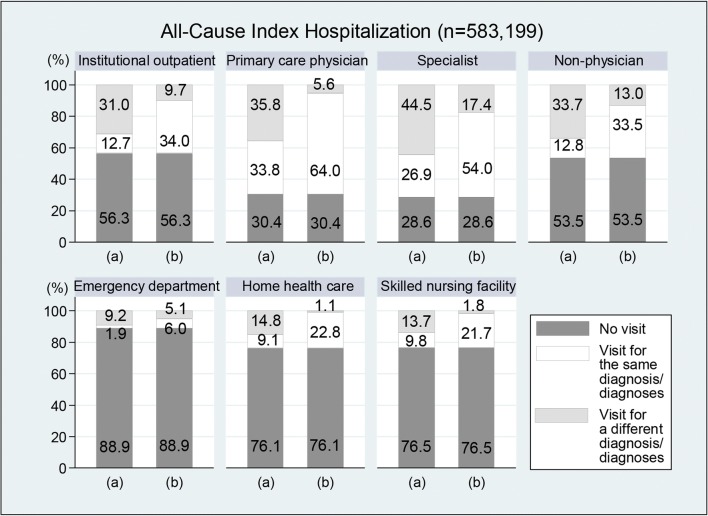
Design and participants: The study sample included 583,199 all-cause IHs among 2014 Medicare fee-for-service beneficiaries. For all-cause IH, as well as individually for heart failure, myocardial infarction, and pneumonia IH, we used multivariable logistic regressions to investigate the association between post-discharge services utilization and readmission.
Main measures: The outcome was unplanned 30-day readmission. Primary independent variables were post-discharge services utilization, including institutional outpatient, office-based primary care, office-based specialist, office-based non-physician practitioner, emergency department, home health care, and skilled nursing facility providers.
Key results: Among all-cause IH, 11.7% resulted in unplanned 30-day readmissions, and only 18.1% of readmissions occurred for the same primary diagnosis as IH. A substantial majority of post-discharge health services were utilized for a primary diagnosis differing from IH. Compared with no visit, institutional outpatient visits for the same primary diagnosis as IH (odds ratio [OR], 0.33; 95% confidence interval [CI], 0.31-0.34) and for a different primary diagnosis than IH (OR, 0.36; 95% CI, 0.35-0.37) were similarly strongly associated with decreased unplanned 30-day readmission. Primary care physician, specialist, non-physician practitioner, and home health care showed similar patterns. IH for heart failure, myocardial infarction, and pneumonia manifested similar patterns to all-cause IH both in terms of post-discharge services utilization and in terms of its impact on readmission.
Conclusions: To reduce unplanned 30-day readmission more effectively, discharge planning should include post-discharge services to address health conditions beyond the primary cause of the IH.
Keywords: 30-day readmission; Hospital Readmission Reduction Program; all-cause index hospitalization; post-discharge services utilization; service diagnosis.
Conflict of interest statement
The authors declare that they do not have a conflict of interest.
Figures
Similar articles
-
Association of Post-discharge Service Types and Timing with 30-Day Readmissions, Length of Stay, and Costs.J Gen Intern Med. 2021 Aug;36(8):2197-2204. doi: 10.1007/s11606-021-06708-6. Epub 2021 May 13. J Gen Intern Med. 2021. PMID: 33987792 Free PMC article.
-
Current Risk Adjustment and Comorbidity Index Underperformance in Predicting Post-Acute Utilization and Hospital Readmissions After Joint Replacements: Implications for Comprehensive Care for Joint Replacement Model.Arthritis Care Res (Hoboken). 2017 Nov;69(11):1668-1675. doi: 10.1002/acr.23195. Epub 2017 Oct 9. Arthritis Care Res (Hoboken). 2017. PMID: 28118530 Free PMC article.
-
Diagnoses and timing of 30-day readmissions after hospitalization for heart failure, acute myocardial infarction, or pneumonia.JAMA. 2013 Jan 23;309(4):355-63. doi: 10.1001/jama.2012.216476. JAMA. 2013. PMID: 23340637 Free PMC article.
-
Impact of Hospital Readmissions Reduction Program Policy on 30-Day and 90-Day Readmissions in Patients With Acute Myocardial Infarction: A 10-Year Trend From the National Readmissions Database.Curr Probl Cardiol. 2023 Jul;48(7):101696. doi: 10.1016/j.cpcardiol.2023.101696. Epub 2023 Mar 14. Curr Probl Cardiol. 2023. PMID: 36921652 Review.
-
The Hospital Readmissions Reduction Program: Nationwide Perspectives and Recommendations: A JACC: Heart Failure Position Paper.JACC Heart Fail. 2020 Jan;8(1):1-11. doi: 10.1016/j.jchf.2019.07.012. Epub 2019 Oct 9. JACC Heart Fail. 2020. PMID: 31606360 Review.
Cited by
-
Usefulness of a Nurse-Led Program of Care for Management of Patients with Chronic Heart Failure.Med Sci Monit. 2020 Feb 18;26:e920469. doi: 10.12659/MSM.920469. Med Sci Monit. 2020. PMID: 32068197 Free PMC article.
-
Awareness of and subjective needs for post-discharge healthcare services among older adult patients.BMC Nurs. 2023 Apr 18;22(1):129. doi: 10.1186/s12912-023-01247-3. BMC Nurs. 2023. PMID: 37072840 Free PMC article.
-
Luck of the draw: Role of chance in the assignment of medicare readmissions penalties.PLoS One. 2021 Dec 21;16(12):e0261363. doi: 10.1371/journal.pone.0261363. eCollection 2021. PLoS One. 2021. PMID: 34932592 Free PMC article.
-
Association of Post-discharge Service Types and Timing with 30-Day Readmissions, Length of Stay, and Costs.J Gen Intern Med. 2021 Aug;36(8):2197-2204. doi: 10.1007/s11606-021-06708-6. Epub 2021 May 13. J Gen Intern Med. 2021. PMID: 33987792 Free PMC article.
References
-
- Jencks SF, Williams MV, Coleman EA. Rehospitalizations among patients in the Medicare fee-for-service program. N Engl J Med. 2009;360(14):1418–28. - PubMed
-
- Crosson F, Christianson J, Miller M. Report to the Congress: Medicare and the Health Care Delivery System. Washington, D.C: Medicare Payment Advisory Commission; 2017.
-
- Hansen LO, Young RS, Hinami K, Leung A, Williams MV. Interventions to reduce 30-day rehospitalization: a systematic review. Ann Intern Med. 2011;155(8):520–8. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
