

MET IHC Is a Poor Screen for MET Amplification or MET Exon 14 Mutations in Lung Adenocarcinomas: Data from a Tri-Institutional Cohort of the Lung Cancer Mutation Consortium
- PMID: 31228623
- PMCID: PMC6708730
- DOI: 10.1016/j.jtho.2019.06.009
MET IHC Is a Poor Screen for MET Amplification or MET Exon 14 Mutations in Lung Adenocarcinomas: Data from a Tri-Institutional Cohort of the Lung Cancer Mutation Consortium
Abstract
Introduction: MNNG HOS Transforming gene (MET) amplification and MET exon 14 (METex14) alterations in lung cancers affect sensitivity to MET proto-oncogene, receptor tyrosine kinase (MET [also known by the alias hepatocyte growth factor receptor]) inhibitors. Fluorescence in situ hybridization (FISH), next-generation sequencing (NGS), and immunohistochemistry (IHC) have been used to evaluate MET dependency. Here, we have determined the association of MET IHC with METex14 mutations and MET amplification.
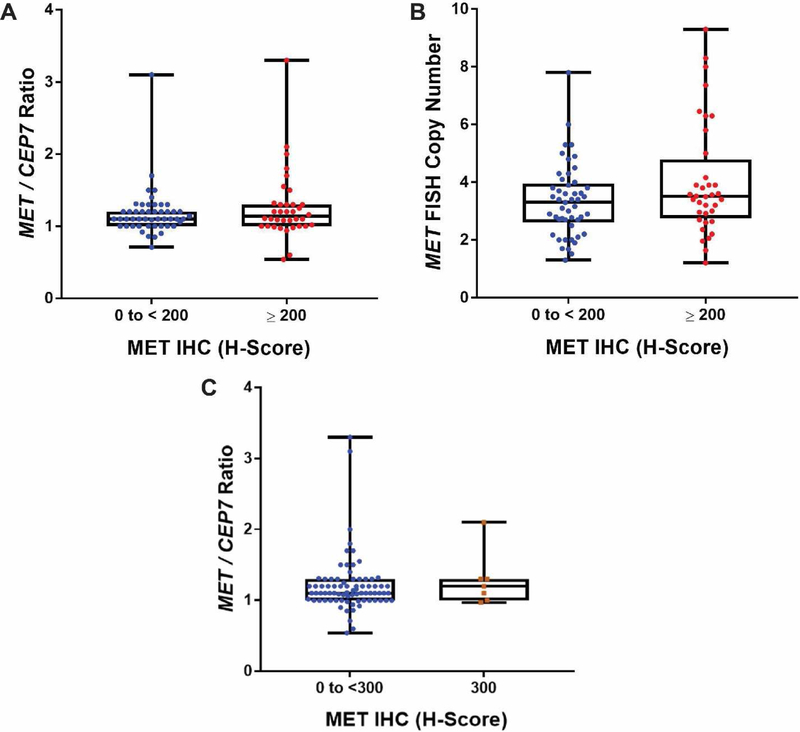
Methods: We collected data on a tri-institutional cohort from the Lung Cancer Mutation Consortium. All patients had metastatic lung adenocarcinomas and no prior targeted therapies. MET IHC positivity was defined by an H-score of 200 or higher using SP44 antibody. MET amplification was defined by copy number fold change of 1.8x or more with use of NGS or a MET-to-centromere of chromosome 7 ratio greater than 2.2 with use of FISH.
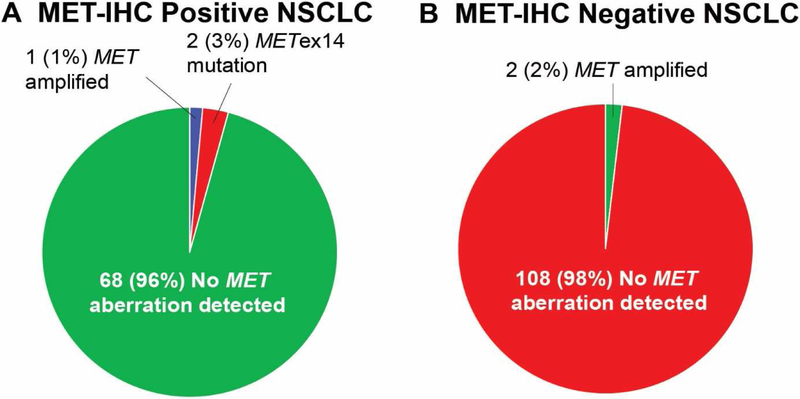
Results: We tested tissue from 181 patients for MET IHC, MET amplification, and METex14 mutations. Overall, 71 of 181 patients (39%) were MET IHC-positive, three of 181 (2%) were MET-amplified, and two of 181 (1%) harbored METex14 mutations. Of the MET-amplified cases, two were FISH positive with MET-to-centromere of chromosome 7 ratios of 3.1 and 3.3, one case was NGS positive with a fold change of 4.4x, and one of the three cases was MET IHC-positive. Of the 71 IHC-positive cases, one (1%) was MET-amplified and two (3%) were METex14-mutated. Of the MET IHC-negative cases, two of 110 (2%) were MET-amplified.
Conclusions: In this study, nearly all MET IHC-positive cases were negative for MET amplification or METex14 mutations. MET IHC can also miss patients with MET amplification. The limited number of MET-amplified cases in this cohort makes it challenging to demonstrate an association between MET IHC and MET amplification. Nevertheless, IHC appears to be an inefficient screen for these genomic changes. MET amplification or METex14 mutations can best be detected by FISH and a multiplex NGS panel.
Keywords: FISH; Immunohistochemistry; Lung cancer; MET exon 14; MET-amplified; Next-generation sequencing.
Copyright © 2019 International Association for the Study of Lung Cancer. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Wu YL, Zhang L, Kim DW, et al. Phase Ib/II Study of Capmatinib (INC280) Plus Gefitinib After Failure of Epidermal Growth Factor Receptor (EGFR) Inhibitor Therapy in Patients With EGFR-Mutated, MET Factor-Dysregulated Non-Small-Cell Lung Cancer. J Clin Oncol 2018:JCO2018777326. - PubMed
-
- Camidge DR, Otterson GA, Clark JW, et al. Crizotinib in patients (pts) with MET-amplified non-small cell lung cancer (NSCLC): Updated safety and efficacy findings from a phase 1 trial. . Journal of Clinical Oncology 2018:Abstr 9062.
-
- Reungwetwattana T, Liang Y, Zhu V, et al. The race to target MET exon 14 skipping alterations in non-small cell lung cancer: The Why, the How, the Who, the Unknown, and the Inevitable. Lung Cancer 2017;103:27–37. - PubMed
-
- Felip E, Horn L, Patel JD, et al. Tepotinib in patients with advanced non-small cell lung cancer (NSCLC) harboring MET exon 14-skipping mutations: Phase II trial. Journal of Clinical Oncology 2018;36:9016–9016.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
