

Mapping the global endemicity and clinical burden of Plasmodium vivax, 2000-17: a spatial and temporal modelling study
- PMID: 31229233
- PMCID: PMC6675736
- DOI: 10.1016/S0140-6736(19)31096-7
Mapping the global endemicity and clinical burden of Plasmodium vivax, 2000-17: a spatial and temporal modelling study
Abstract
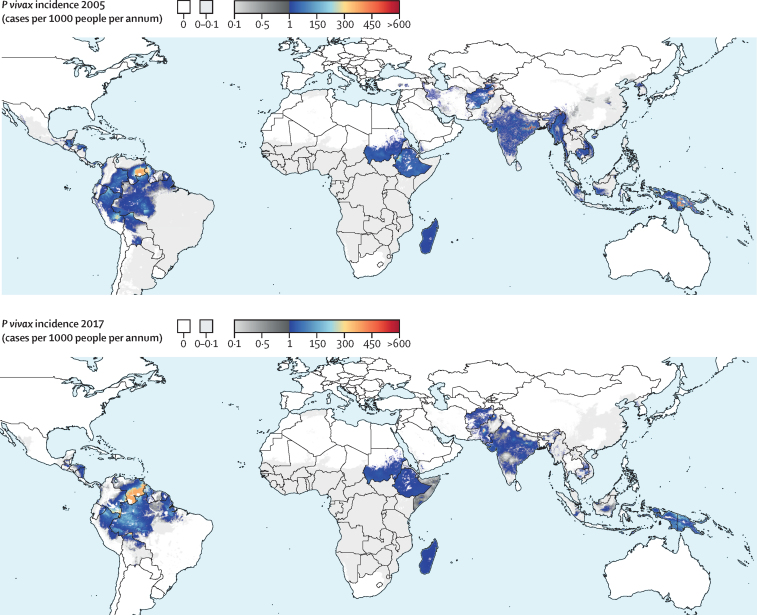
Background: Plasmodium vivax exacts a significant toll on health worldwide, yet few efforts to date have quantified the extent and temporal trends of its global distribution. Given the challenges associated with the proper diagnosis and treatment of P vivax, national malaria programmes-particularly those pursuing malaria elimination strategies-require up to date assessments of P vivax endemicity and disease impact. This study presents the first global maps of P vivax clinical burden from 2000 to 2017.
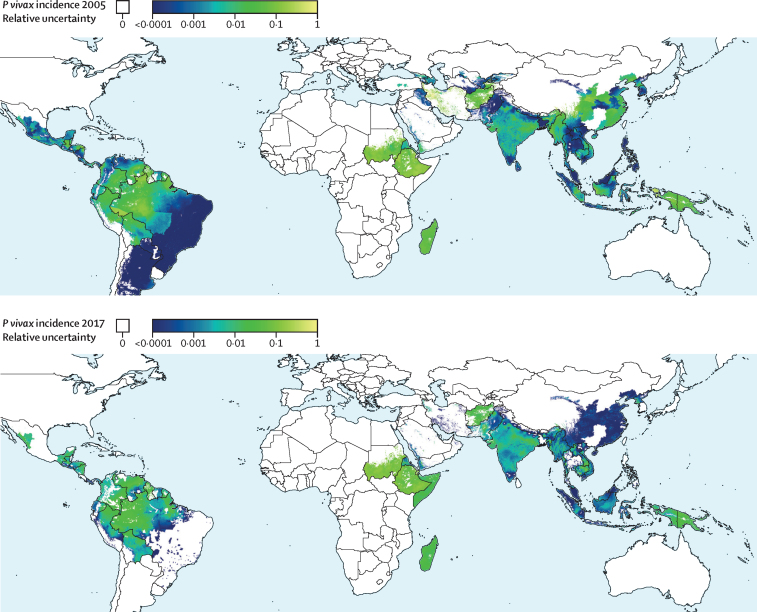
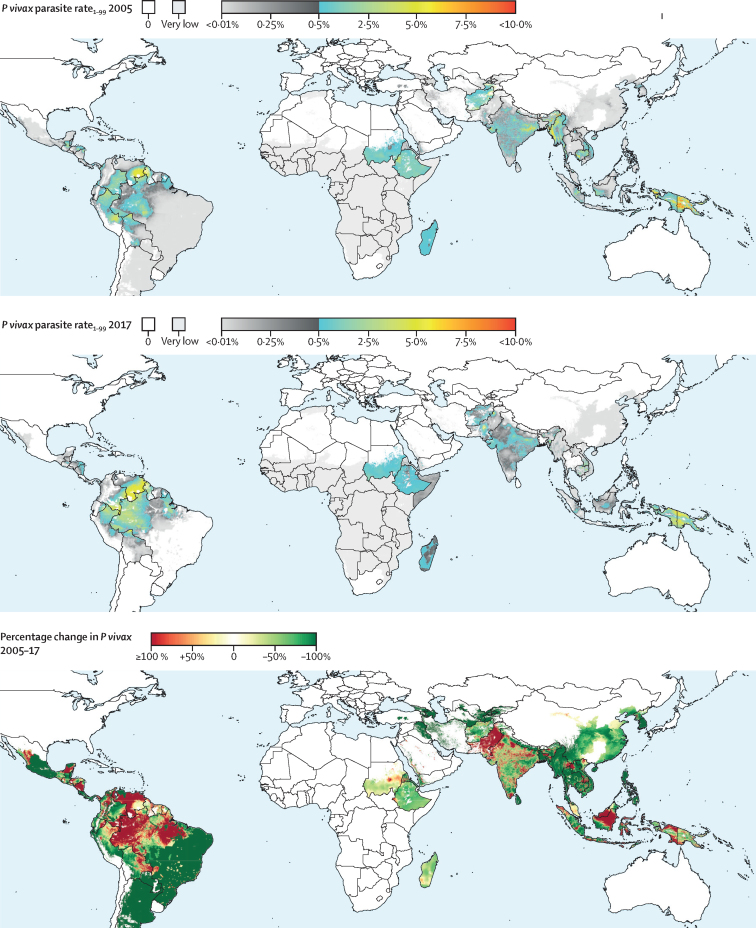
Methods: In this spatial and temporal modelling study, we adjusted routine malariometric surveillance data for known biases and used socioeconomic indicators to generate time series of the clinical burden of P vivax. These data informed Bayesian geospatial models, which produced fine-scale predictions of P vivax clinical incidence and infection prevalence over time. Within sub-Saharan Africa, where routine surveillance for P vivax is not standard practice, we combined predicted surfaces of Plasmodium falciparum with country-specific ratios of P vivax to P falciparum. These results were combined with surveillance-based outputs outside of Africa to generate global maps.
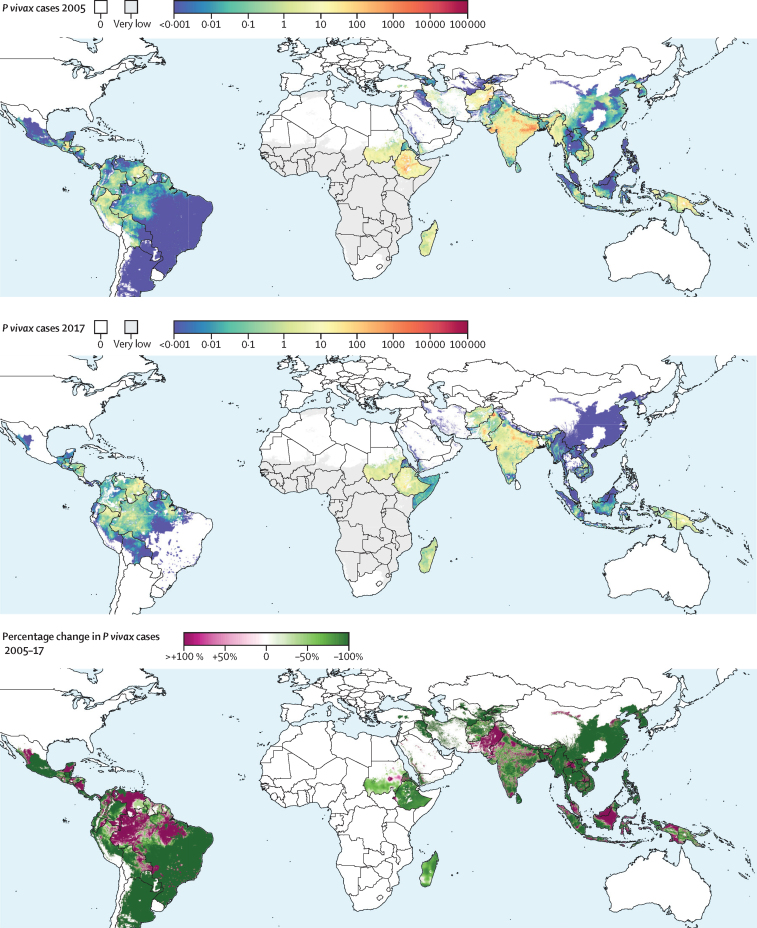
Findings: We present the first high-resolution maps of P vivax burden. These results are combined with those for P falciparum (published separately) to form the malaria estimates for the Global Burden of Disease 2017 study. The burden of P vivax malaria decreased by 41·6%, from 24·5 million cases (95% uncertainty interval 22·5-27·0) in 2000 to 14·3 million cases (13·7-15·0) in 2017. The Americas had a reduction of 56·8% (47·6-67·0) in total cases since 2000, while South-East Asia recorded declines of 50·5% (50·3-50·6) and the Western Pacific regions recorded declines of 51·3% (48·0-55·4). Europe achieved zero P vivax cases during the study period. Nonetheless, rates of decline have stalled in the past five years for many countries, with particular increases noted in regions affected by political and economic instability.
Interpretation: Our study highlights important spatial and temporal patterns in the clinical burden and prevalence of P vivax. Amid substantial progress worldwide, plateauing gains and areas of increased burden signal the potential for challenges that are greater than expected on the road to malaria elimination. These results support global monitoring systems and can inform the optimisation of diagnosis and treatment where P vivax has most impact.
Funding: Bill & Melinda Gates Foundation and the Wellcome Trust.
Copyright © 2019 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Figures

Comment in
-
New malaria maps.Lancet. 2019 Jul 27;394(10195):278-279. doi: 10.1016/S0140-6736(19)31273-5. Epub 2019 Jun 19. Lancet. 2019. PMID: 31229232 No abstract available.
References
-
- Gates B, Chambers R. From Aspiration to Action. 2015. http://endmalaria2040.org/
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
