

Adjuvant Therapy for Node-Positive Esophageal Cancer After Induction and Surgery: A Multisite Study
- PMID: 31229485
- PMCID: PMC6904117
- DOI: 10.1016/j.athoracsur.2019.04.099
Adjuvant Therapy for Node-Positive Esophageal Cancer After Induction and Surgery: A Multisite Study
Abstract
Background: The benefit of adjuvant treatment for esophageal cancer patients with positive lymph nodes after induction therapy and esophagectomy is uncertain. This in-depth multicenter study assessed the benefit of adjuvant therapy in this population.
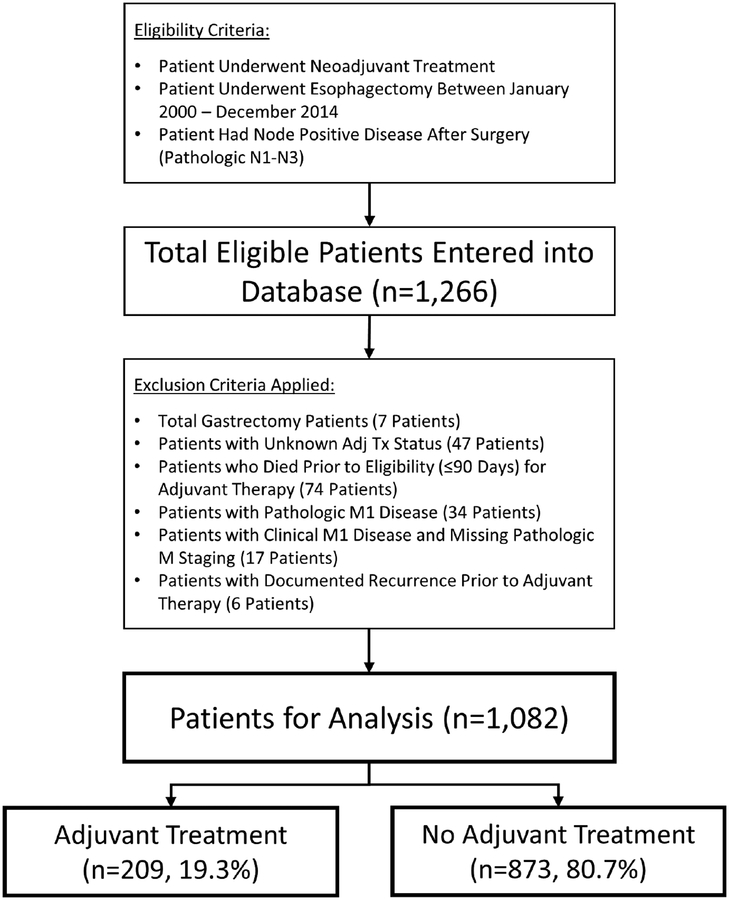
Methods: A retrospective cohort study from 9 institutions included patients who received neoadjuvant treatment, underwent esophagectomy from 2000 to 2014, and had positive lymph nodes on pathology. Factors associated with administration of adjuvant therapy were assessed using multilevel random-intercept modeling to account for institutional variation in practice. Kaplan-Meier analyses were performed based on adjuvant treatment status. Variables associated with survival were identified using Cox proportional hazards modeling.
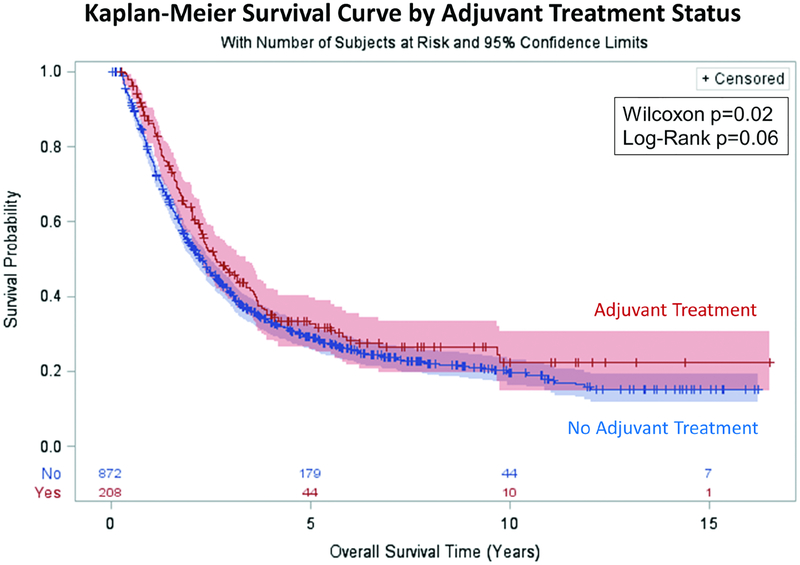
Results: The study analyzed 1082 patients with node-positive cancer after induction therapy and esophagectomy: 209 (19.3%) received adjuvant therapy and 873 (80.7%) did not. Administration of adjuvant treatment varied significantly from 3.2% to 50.0% between sites (P < .001). Accounting for institution effect, factors associated with administration of adjuvant therapy included clinically positive and negative prognostic characteristics: younger age, higher pathologic stage, pathologic grade, no neoadjuvant radiotherapy nonsmoking status, and absence of postoperative infection. Kaplan-Meier analysis showed patients receiving adjuvant therapy had a longer median survival of 2.6 years vs 2.3 years (P = .02). Cox modeling identified adjuvant treatment as independently associated with improved survival, with a 24% reduction in mortality (hazard ratio, 0.76; P = .005).
Conclusions: Adjuvant therapy was associated with improved overall survival. Therefore, consideration should be given to administration of adjuvant therapy to esophageal cancer patients who have persistent node-positive disease after induction therapy and esophagectomy and are able to tolerate additional treatment.
Copyright © 2019 The Society of Thoracic Surgeons. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Farjah F, Gerdes H, Gibson M, Glasgow RE, Hayman JA, et al. NCCN Guidelines Version 2.2018 Esophageal and Esophagogastric Junction Cancers NCCN Evidence Blocks™. 2018.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
